|
|
|
|
|
|
|
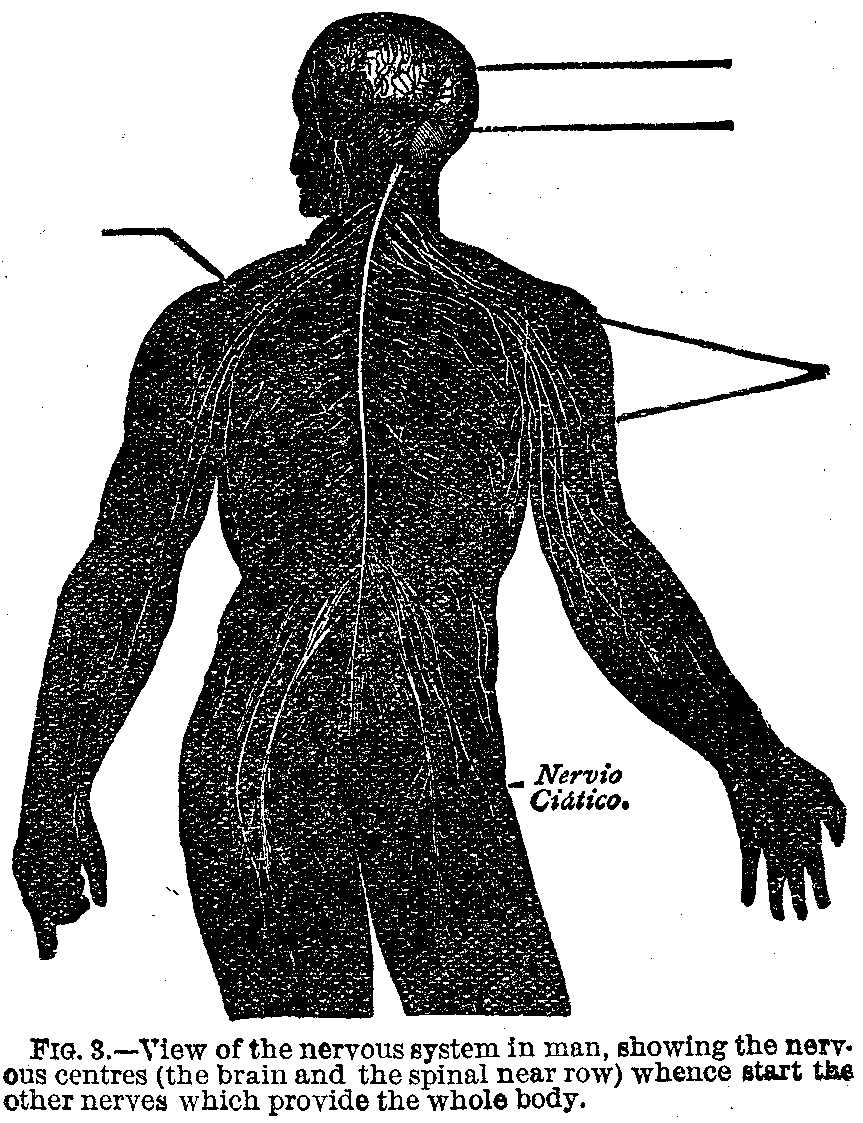
Division of Nerves.—1. Motor nerves or those in which irritation produces muscular contraction.
2. Sensitive nerves, or nerves of common sensibility, in which irritation is followed by an agreeable or painful feeling, according to the nature or degree of the stimulation.
3. Nerves of special sense in which irritation excites the peculiar sensations of light, sound, taste, etc. Many sensitive nerves arise from nervous centres in such close proximity to motor nerves that a stimulus applied to the former will react upon the latter and produce not only a direct sensation, but what is technically called a reflex action. It is a remarkable fact that whatever part of a sensitive nerve be irritated, whether it be the centre, the middle, or the extremity, the same sensation will be produced.
Nature of Nervous Force.—We can judge of the nature of the nervous force only by its effects. The muscular contraction caused by the irritation of a nerve is due to the development of a peculiar vital force in the nerve structure, which is unlike any of the known physical forces. It bears certain analogies to electricity.
1. The identity of their effects on muscular fibre.
2. The rapidity of their action without producing any appreciable effect on the parts between the point of irritation and the point affected.
3. The extreme sensibility of nerves to the electric current.
4. The phenomena of electrical fishes.
Peculiarity.—It is the consequence of chronic or acute inflammation, or it may occur from obliteration of the arteries.
Softening of the mucous membrane of the digestive organs is of much more frequent occurrence than softening of the brain.
Causes.—Two causes appear to cooperate in producing softening of the brain. The first is of a mechanical, the second of a physiological nature. Serosity, or pus, when in considerable quantity, appear to effect, mechanically, a diminution of the cohesion of the tissue in which they are contained. The pressure which they exercise arrests the circulation, and it would appear absorption also; for if this function were performed we should have an excavation or ulcer formed instead of a mass of soft pulpy tissue. The circulation being thus arrested nutrition ceases to be accomplished and the molecules of the tissues are disunited and detached. If while these changes are going on, or at some subsequent period, the function of absorption be resumed, the softened tissue is partially or wholly absorbed and solutions of continuity of various extent are formed. The physiological cause, therefore, of softening is referable to a change in the vital properties of the affected tissue.
|
|
|
|
|
|
|
Degree of Softening.—The degree of softening of the cerebral substance may vary from a slight diminution of the natural consistence of the part to that of cream or even of thin milk. The first stage of softening of this substance is often so slight that it is hardly perceptible to the touch, and may, even when considerable, if not accompanied by some peculiarity of color, be altogether overlooked.
Physical Characters.—The color of inflammatory softening of the cerebral substance presents considerable variety, dependent on the quantity of blood contained in the affected part. Redness and vascularity are, in general, greater in the first than in the second stage, but the degree and extent of either greatly depend on the quantity of blood in the cerebral vascular system. When the redness which accompanies softening arises from the presence of effused blood it may always be regarded as evidence that the softening is of recent occurrence.
Other Evidences of Softening.—But there are other modifications of color which accompany softening of the cerebral substance. They indicate that the disease has existed for a considerable time, several weeks, or two or three months. The principal modifications of color consist of brown, yellow and orange, either separately or combined, and occupy either the softened substance, the part of the brain contiguous to it, or both at the same time. They are not observed unless the softening has been accompanied by effusion and originate in changes taking place in the effused blood.
When Softening May Occur.—Softening may occur in the brain and medullary substances at the same time. It may also occupy several portions of the brain at the same time, as the septum lucidum, fornix and walls of the lateral ventricles, the corpora striata and thalami, one or more lobes, a portion of one or both hemispheres, the brain and cerebellum, and is rarely met with in the latter organ without its being present in the former. Circumstances which give great variety and complexity to the functional derangement by which it is accompanied.
|
|
|
|
|
|
|
Symptoms.—As the symptoms of the first period of inflammatory softening of the brain must necessarily be those of inflammation of this organ, it would be superfluous to describe them here. It may, however, be observed that the severity of these symptoms does not always indicate a corresponding condition as to the extent of the softening which they precede, nor do they present any one character which can be regarded as a sign that the inflammation on which they depend will terminate in softening. When, however, they are taken in conjunction with those of the second period, they are frequently of great value as they afford us the means of establishing our diagnosis in cases where it would be otherwise impossible.
Symptoms of Second Period.—The symptoms of the second period of inflammatory softening of the brain are of an entirely opposite character to those of the first period. Those of the first depending on the presence of irritation, or a morbid stimulus, are characterized by a state of excitement; whereas those of the second being the consequence of the softening or disorganiztion of the cerebral substance, are necessarily marked by a state of prostration, collapsus or paralysis. They are announced by the gradual or sudden diminution of the intellectual powers, by the occurrence of stupor or coma, by paralysis, difficulty or loss of speech and diminution of the sensibility of the skin, eye and ear. The relative frequency, degree and extent of these symptoms, as well as the order of their occurrence, present considerable variety. Thus, the derangement of the intellectual faculties, such as their diminution, suspension or abolition, is always present at the commencement of the second period, that is so soon as the softening of the cerebral substance has taken place. In some cases the derangement which they manifest is at first slight, increases gradually or rapidly and terminates in their entire abolition. In others these faculties are, from the commencement, gravely compromised and give no signs whatever of their existence.
Peculiar Symptoms.—It is not rare to meet with cases in which their derangement is marked by remissions and exacerbations, or the occurrence of lucid intervals succeeded by profound stupor. The delirium which accompanies the first period of inflammatory softening either disappears or diminishes greatly in intensity when the second period is announced by the derangement of the intellectual faculties to which we have alluded. It diminishes with the diminution of these faculties and ceases when their suspension or abolition is indicated by the presence of coma and complete paralysis.
|
|
|
|
|
|
|
Loss of Memory.—An imperfect state or the entire loss of memory and speech are necessary consequences of these latter conditions of the intellectual faculties. But the absence of any derangement of these faculties is not necessarily unaccompanied by derangement of memory and speech, particularly the latter, for a patient may recover the consciousness of his existence, perceive and comprehend what is passing around him, and yet be incapable of expressing himself in words on account of paralysis of the muscles by means of which the act of speech is accomplished. The diminution, suspension or abolition of the intellectual functions are always accompanied with paralysis of the muscles of voluntary motion, and the degree of the paralysis is, generally, in the direct ratio of the extent of the derangement manifested by these functions.
Brain Paralysis.—The paralysis is rarely complete at the commencement. It is generally progressive with occasional alternations of increase and decrease before it becomes ultimately complete. The situation and extent of the paralysis present considerable variety and in many cases seem to correspond with the situation and extent of the softening, in the same manner as in apoplexy. The paralysis occupies one or both extremities of the same side when the softening is limited to one of the hemispheres of the brain, and paraplegia or universal paralysis is produced when both hemispheres, the pons varolii, etc., are the seat of this lesion. Paralysis occurs more frequently in the superior than in the inferior extremities; the seat of the lesion of the former being in the corpus striatum, and of the latter, the optic thalamus of the opposite side of the brain.
Paralysis of Face Muscles.—Paralysis of the muscles of the face, of the eye, of the tongue and of deglutition, depends likewise in the situation of the softening. Paralysis of the bladder and rectum is a frequent occurrence of softening of the brain, and gives rise, in the first place, to an accumulation of the contents of these organs, and afterward to their involuntary escape, more particularly of the urine, from the distension of the bladder and the subsequent dilatation of its sphincter. It is under similar circumstances of the brain that the organs of hearing and of sight, which in the first inflammatory period of softening are highly susceptible, are rendered obtuse to a degree that a strong light or loud sounds impressed on the eye and ear pass unperceived.
Permanent Muscular Contraction.—One of the most constant symptoms of inflammatory softening of the brain is a state of permanent contraction of the flexor muscles of the extremities.
|
|
|
|
|
|
|
The last symptom which we shall notice is that of pain. This does not depend on the state of softening of the cerebral substance. It is the consequence of irritation or morbid excitement of the brain, the disorganization of which has not yet taken place. It is generally most severe when it occurs as a precursory symptom, but it frequently accompanies the first period of the disease, and presents remissions and exacerbations, variable in duration and degree.
Treatment.—There are no successful cases recorded of softening from obliteration of the arteries, and in the few cases of the inflammatory forms of the disease, which have terminated favorably, it is more than probable that the softening was very limited in extent and affected the superficial or less important parts of the brain. As regards the state of softening, which, in point of fact, consists in a solution of continuity of the cerebral substance, it must be obvious that we possess no remedial agent capable of obviating such a change. The diseased state, therefore, of which we are treating, is incurable; that is to say, the solution of continuity of which it consists will remain, even though the patient should recover. The essential part of the treatment of softening of the brain relates, consequently, to the local morbid conditions which immediately precede this change, viz.: the diseased state of the arteries on the one hand and inflammation of the brain on the other. This state of the arteries, like the softening to which it gives rise, is so far as we yet know, beyond the control of remedial agents. When, therefore, it is ascertained that the softening is the consequence of this state of the arteries, the only hope that can be indulged is partial relief, and the prolongation of life for a short period beyond that at which the disease would have proved fatal had it been allowed to run its natural course.
Staying Treatment.—It is possible that the attack may be delayed by judicious treatment, employed when the first symptoms of cerebral derangement are perceived, such as pain in a particular part of the head, confusion of ideas, giddiness or unusual drowsiness and listlessness, together with a prickling sensation or numbness in the muscles of the extremities, face or tongue.
Further Treatment.—Bleeding from the temples, cupping in the nape of the neck, or small general bleedings, repeated from time to time as circumstances may require, may, by diminishing the quantity of the blood, facilitate the circulation of this fluid through the brain. But, perhaps, the greater advantage would be derived by keeping the bowels freely open
(Continued on page pg0340)
|
|
|
|
|
|
|
FIGURE NO. 1.
1,1,1,1. Motor track delineated from the front columns of
the spinal marrow to the hemispheric ganglion.
2. Pyramidal body.
3. Eminences in the medula oblongata.
4. Variolus bridge.
5. Legs of the brain.
6. Streaked body.
7. Hemispheric ganglion.
8. Cerebellum.
9. Olfactory nerve.
10. Optic nerve.
11. Fourth pair of nerves.
12. Sensory root of the fifth pair.
13. The seventh and eighth pairs of nerves.
14. Front suture.
15. Mammillary elevation.
16. Corpora geniculatum.
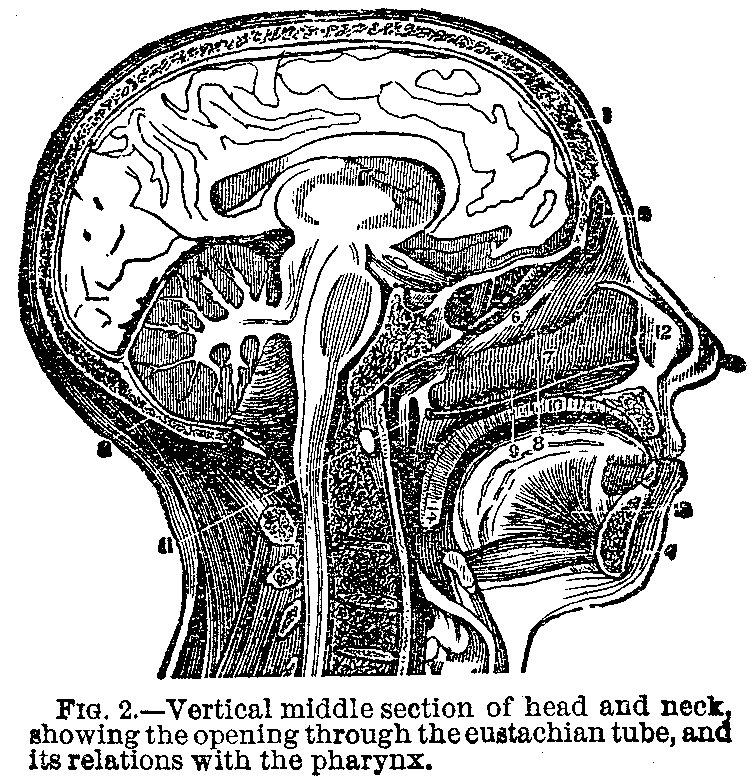
FIGURE NO. 2.
1,1. Section of the callous body.
2. Transparent partition.
3. Front column of the vault.
4. Section of front suture.
5. Central substance of the chamber.
6. Sylvius' aqueduct.
7. Pineal gland.
8. Medullar band which extends from the pineal gland to the front suture.
9. Section of the legs of the brain.
10. One of the white bodies, or mammillary bodies.
11. Gray excrescence.
12. Section of the intricacy of the optic nerves.
13. Optic nerve beyond the intricacy.
14. Olfactory nerve.
15. Front surface of the hemisphere.
16. Fissure between the back and middle lobes of the brain.
FIGURE NO. 3.
1. Front extremity of the fissure of the brain.
2. Back extremity.
3. Front lobes of the brain.
4. Middle lobe.
5. The sylvius fisaure.
6. Back lobe.
7. Infundlbulus point.
8. Its body.
9. White or mammillary bodies.
10. Ash-colored matter.
11. Legs of the brain.
12. Variolus' bridge.
13. Upper end of the medulla oblongata.
14. Back prolongation of the variolas bridge.
15. Middle of the cerebellum.
16. Front part.
17. Back part.
18. Upper part of the spinal marrow.
19. Middle fissure of medulla oblongata.
20. Pyramidal body.
21. Rectiform body.
22. Oval body.
23. Olfactory nerve.
24. Its bulb.
25. Its external root.
26. Its middle root.
27. Itg internal root.
28. Optic nerve beyond the intricacy.
29. The same before the intricacy.
30. Motor of the eye or third pair.
31. Pathetic nerves or fourth pair.
32. Trigeminus or fourth pair.
33. External motor or sixth pair.
34. Facial nerve.
35. Auditive nerve.
36,87,38. Eighth pair.
FIGURE NO. 4.
1. Vertical section of the head.
2. Frontal cavity.
3. Greater falce of the brain.
4. Its origin from the rooster's comb.
5. Its union along the sagital suture.
6. Under or concave edge.
7. Counteraction to the cerebellum store.
8. Cerebellum store.
9. Union to temporal bone.
10. Free edge of same.
11. Tortuous elevations of the front right lobe of the brain.
12. Front extremity of the callous body.
13. Transparent partition.
14. Section of the front suture,
15. Front parts of the vault.
16. The middle of same.
17. Back end.
18. Inner side of the bed.
19. Section of streaked bodies.
20. Side walls of the third ventricle.
21. The dura mater, turned upside down.
22. Section of the internal carotid artery.
FIGURE NO. 5.
1. Front lobe of the brain.
2. Back lobe.
3. Middle lobe.
|
|
|
|
|
|
|

FIG. 1.—View of the course of the front columns of the spinal marrow terminating in the hemispheric ganglions of the brain.

FIG. 2.—Middle vertical section of the callous body. The inner left side of the brain is also seen.
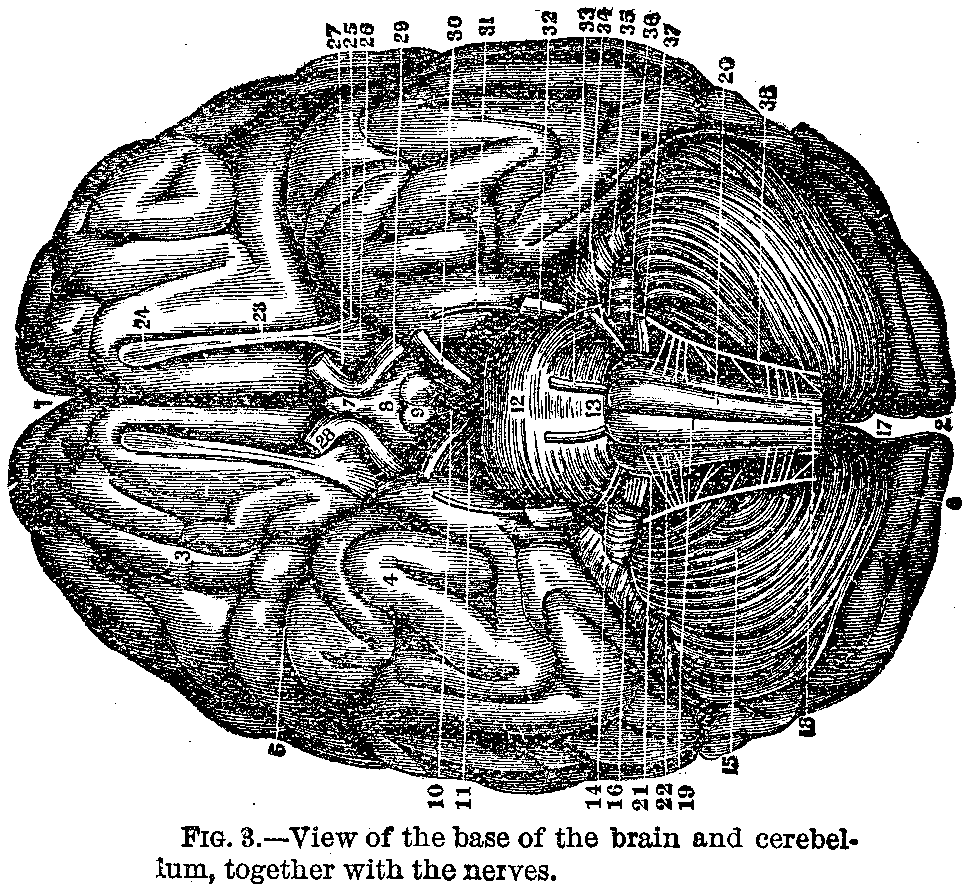
FIG. 3.—View of the base of the brain and cerebellum, together with the nerves.
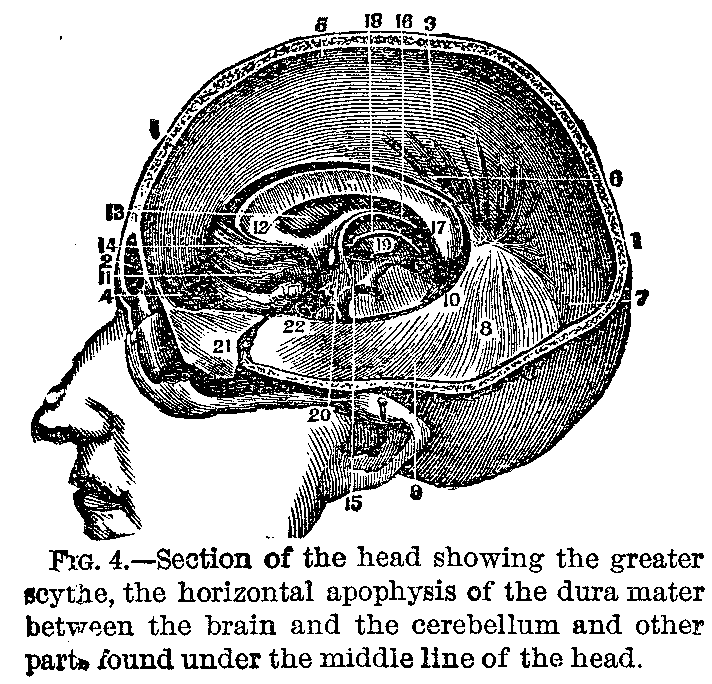
FIG. 4.—Section of the head showing the greater scythe, the horizontal apophysis of the dura mater between the brain and the cerebellum and other parts found under the middle line of the head.
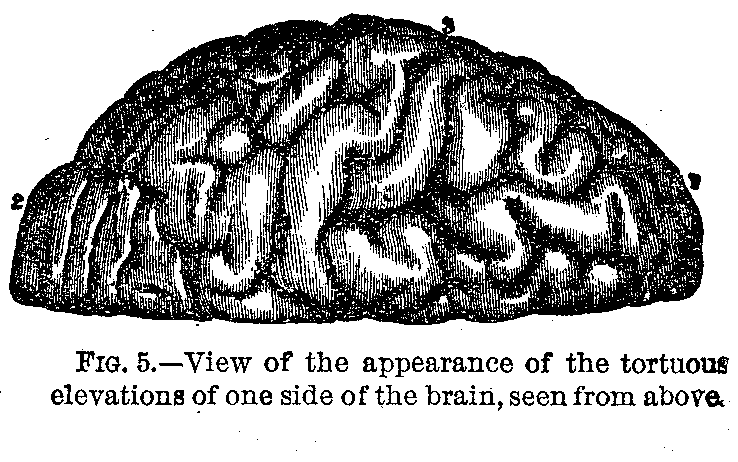
FIG. 5.—View of the appearance of the tortuous elevations of one side of the brain, seen from above.
For an explanation of the illustrations see text on opposite page.
without inducing excitement or debility, chiefly by means of the neutral salts. The compound aloetic pill will be advantageously employed in those cases in which the disease occurs after the cessation of the catamenia, or suppression of a hemorrhoidal discharge. A diminution of the circulating fluids, as well as their equalization, will be effected likewise by promoting all the secretions, particularly those of the urine and bile.
|
|
|
|
|
|
|
Diet.—The food and drink of the patient should be particularly attended to. His diet should consist of those kinds of food which are most easily digested, and which afford the greatest quantity of nourishment in the smallest bulk. Ardent spirits, strong wines, fermented liquors; even strong coffee or tea and all stimulants should be avoided as more or less injurious.
Treatment of Second Period.—The treatment of the second period, or that of softening from inflammation, is the same in principle as that of the former, in so far as it regards the state of excitement with which this morbid change is generally accompanied. But if the paralysis be fairly established and, notwithstanding the depletory and sedative measures which have been employed, continues to increase, neither our own observation nor the recorded experience of others would recommend a steady perseverance in the means, the debilitating effects of which have not been sufficient to overcome the inflammatory excitement of the first period. Bleeding and active purgatives should now be laid aside; blisters or sinapism should be applied to the inferior extremities, the nape of the neck and superior part of the spine; the head should be kept cool by the constant application of evaporating lotions; the bowels evacuated once or twice a day by means of a mild aperient, or by injections, the secretion of urine and the cutaneous perspiration should also be promoted by remedies of the least stimulating qualities. The retention of the urine is a complication which must be sedulously watched, that this fluid may be removed before it accumulates to a degree to prove injurious; stimuli or tonics should now be employed with a view to support the strength of the patient, but they ought never to be employed to such an extent as to produce excitement, as the powers of life are already greatly exhausted by the stimulus of the disease.
(Cerebral Macula)
Difficult Diagnosis.—Under this term we propose to include the pathology, symptoms and treatment of the inflammatory affections of the brain and of its membranes. We adopt this plan, not merely because of the intimate relation subsisting between these structures, but because, when we trace the history of a number of acute affections of the encephalon and examine the lesions of structure presented after death, we shall frequently find that the substance of the organ, as well as the investing membranes, has been involved in the disease. Hence arises the difficulty of establishing the diagnosis between inflammation of the parenchyma of the brain and that of its membranes.
|
|
|
|
|
|
|
Symptoms.—When either the arachnoid or pia mater, which closely invest the brain, are extensively inflamed, the functions of this organ become inevitably disturbed by sympathetic irritation, without its parenchyma necessarily partaking of the inflammation, or if the inflammation extends to the parenchyma it is mostly confined to the superficial layer of cortical substance. Hence meningitis, beside headache and intense fever, we have an increase of the general sensibility, preternatural acuteness of the external senses, violent delirium and convulsions, and, finally, collapse, coma and death. Extensive and acute inflammation of the hemispheres of the brain will be characterized by a nearly similar train of symptoms.
Two Classes of Inflammation.—We shall proceed to consider inflammation of the encephalon under two divisions, viz.: 1. Inflammation of the membranes of the brain (meningitis); 2. Inflammation of the substance of the brain (cerebritis).
Inflammation of Brain Membrane.—An examination of the structure of the brain and of the peculiarities of the circulation in it and upon it would lead us to the inference that if the meninges be the seat of inflammation, the contiguous cerebral substance must participate in some degree in the irritative influence. In other organs the vessels, after entering them by trunks and branches of various sizes, branch out and ramify in their interior until they become capillary in their spongy and areolar tissue. But in the brain a different arrangement takes place, the vessels, after entering at the base of the skull, communicate freely with one another and then branch out upon the surface of the brain, ramifying in an extended web or cellular tissue (pia mater); in this way they become reduced to so great a degree of tenuity before they enter the substance of the organ that it may be said to be surrounded by a vascular atmosphere from which its supplies are derived. Hence it is, that as the meninges and the contiguous cerebral substance are supplied from the same source, each will more or less become affected by any inflammatory action set up in the other.
Sympathetic Symptoms.—Cerebral irritations are divisible into two great classes, symptomatic and idiopathic. Symptomatic irritation is for the most part connected with and dependent as a morbid condition of the chylopoetic viscera. We frequently observe that for weeks previously to the occurrence of pain or any disturbance in the head the digestive functions have been impaired, the bowels confined or irregular and the stools unnatural. In many of these cases, when the headache, retching, irregular fever and even coma have set in, speedy and permanent relief has followed the use of purgatives, and the other means usually resorted to for correcting disordered functions. An irritative influence is in such cases propagated from the digestive organs to the brain by reason of the close sympathetic connection which subsits between them in health and in disease, and that irritation, if kept up for a while, will pass into positive inflammation, marked by its usual consequences. The irritation of worms and of teething may also induce similar results, more particularly in those constitutionally predisposed. We frequently observe these cerebral affections to spring up during the course of other diseases, of which they may be considered as complications, viz.: continued fever, scarlatina, measles, whooping-cough, and they not unfrequently follow accidents or injuries.
|
|
|
|
|
|
|
Varying Symptoms.—This affection presents a train of symptoms which varies in different ages and in different temperaments. Its most marked and ordinary character at its outset is an increased sensibility to all sorts of impressions, the ordinary external influences producing inordinate effects. Thus, a child is restless and sleepless, seldom even dozing, or if he does doze from time to time starting and waking up; he attends to every sound, the eyes are suffused, the retina is so sensitive to light that he winks or turns away if his face is directed to a window or to a light; the pupil is generally contracted but not invariably so. The head is often moved about or from side to side, so are the limbs; the temper is peevish and nothing seems to soothe this irritable condition but motion up and down the room in the arms of the nurse or attendant.
Bowel Symptoms.—The state of the bowels varies much in different instances, they may be confined or relaxed, but the stools do not present any unnatural appearance.
Increased Animation.—There is a minor degree of this state which is marked by increased animation and liveliness, which with ordinary observers may pass for an increase of health and vigor, though an attentive observer will readily perceive that the countenance wants that disengaged air which exists in health, and on making a closer examination he will find that the eyes frequently close and wink and the countenace assumes an expression as of frowning; the hand, too, is frequently raised toward the head, and the fingers are fixedly closed.
|
|
|
|
|
|
|
Indifference.—We occasionally observe a state the very opposite of this, a state characterized by want of animation, accompanied by plaintive moaning at times, and an indifference to surrounding objects. Though the patient does not sleep, yet his state is not that of waking, and if roused, betrays fretfulness and peevishness. These may be considered as so many indications of an incipient irritation, which in some constitutions may arise independently of any assignable agency, but which in many cases is referable to an irritation propagated to the brain from the peripheral extremities of the nerves during dentition, or by worms in the alimentary canal, or by vitiated secretions, or a torpid liver.
Fever Symptoms.—The symptoms above indicated are by some denominated fever, some epithet being usually added for the purpose of indicating its source, or its nature; hence the terms gastric, irritative and hydrocephalic fever.
Morbid Excitement.—The most expressive term which we can employ is that of "sensitive erethism," or morbid excitement. It is distinct from inflammation of the brain, of which it is frequently the precursor, and according to individual peculiarities, or other modifying circumstances, it may end in cerebritis, meningitis or that modification of the latter called hydrocephalus, and this termination is but too often unexpected by the practitioner, whose attention has perhaps been directed to secondary indications and minor effects, while the erethismal state of the brain has crept on unheeded. The condition here indicated cannot be supposed to exist unaccompanied by an increased flow of blood through the cerebral vessels, or in other words, an increase in their degree of tension; and as the tension may vary from a slight degree of fullness to the greatest of which the vessels are susceptible, such a state of local determination of blood will soon end in inflammation if not subdued by proper means.
Further Symptoms.—The actual inflammatory attack is generally ushered in by headache more or less violent (the pain being referred to the temples, the vertex or forehead, sometimes to the occiput and base of the skull), by intolerance of light, heavy and suffused eye, with quick pulse, are also attendants; so, in many instances, is vomiting. In those who have suffered much from mental disquiet spasmodic twitchings are sometimes perceived, not unlike those which arise from slight electric sparks. In children and very young persons it frequently commences with a sudden and long-continued convulsion without any previous warning. After a while the convulsive movements cease, a remission takes place and the patient appears free from complaint for one or more days, when a second attack occurs which may terminate in coma and death.
|
|
|
|
|
|
|
Changes in Membrane.—After having been the subject of inflammation the membranes present various changes dependent either on the duration and intensity of the attack or on the frequency of its recurrence; but all of them are referable to the following heads, viz.: simple redness of the arachnoid; thickening and opacity with increased firmness; serous effusion beneath or upon it or into the ventricles; puriform or sero-purulent exudations; false membranes; increased vascularity and thickening of the pia mater. We also find lesions consisting of granulations scattered in the meninges over the surface of the brain and in the sylvan fissure, which have been shown by the microscope to be of a tubercular nature.
The Delirium.—Meningitis is in many instances so slow in its progress as to assume the chronic form. We have then delirium and progressive paralysis as constant attendants. The delirium is at first partial, it is a monomania with weakness of intellect, but, after a time it passes on to maniacal excitement and finally subsides into confirmed idiocy. The paralysis in those cases does not exhibit a total privation of sensation and motion in any particular part of the body; it is at first slight, but gradually increases and extends to the whole muscular system, rendering the gait feeble and vacillating and ultimately destroying the power of motion. It is remarkable that the diminution of sensation is not proportioned to that of motion. Spasmodic movements with contraction and rigidity of the limbs sooner or later set in, and, finally, epileptic attacks, which terminate in fatal apoplexy.
The Paralysis.—The paralysis which occurs presents this remarkable feature, that it seems to shift about from one hour to the other, one day, for instance, the right leg is found to be drawn up with greater energy than the left, when the sole of the right foot is tickled, but on repeating the examination a few days afterward it is the left leg which now feels and moves better than the right. It would seem from this as if the paralysis had shifted from one side to the other, but such is not the case, the limb which was first palsied is still so, but the illusion arises from the circumstance that the palsy has not increased in degree in the first limb, while the second limb has become involved to a greater degree. Motor power has not returned in the former, but has been more gravely impaired in the latter.
After-Death Facts.—The lesions which are found after death subsequently account for these facts. When the right limbs alone were paralyzed the brain is found to be disorganized on the left side; but when the paralysis apparently shifted from one side to the other both hemispheres are found diseased, but more deeply and more extensively on the opposite side to that of the limbs which were most palsied. This apparent mobility of paralytic symptoms more frequently occurs in meningitis than in any other complaint.
|
|
|
|
|
|
|
Causes.—Meningitis is a frequent consequence of injuries of the head, of fractures, concussion or even wounds of the scalp. It not infrequently happens that a wound of the head heals rapidly and that the patient returns to his usual occupation thinking himself quite well, but after ten or fourteen days he begins to feel pain in the situation of the wound which gradually increases in intensity, and in a very short time all the symptoms of cerebral inflammation become manifest. A child may suffer serious injury from a fall, and as all mention of the accident is suppressed by his immediate attendant, It escapes the notice of others and no ill effects follow perhaps for a week or two; the child then, however, loses appetite, becomes restless and irritable, febrile excitement, delirium and convulsions succeed and too often are the precursors of a fatal termination.
Symptoms.—The most usual premonitory symptoms are a general uneasiness and restlessness with a tendency to congestion in the head; a sense of weight and fullness; occasional attacks of pain in the head, or of temporary apoplexy or epilepsy; flushing of the face and increased heat of the head; drowsiness and vertigo; preternatural acuteness of the external senses; intolerance of light and optical illusions; contraction of the pupils, strabismus or imperfection of sight; tinnitus aurium or various other noises in the ear; confusion of thought; failure of the memory; mental excitement or depression, or some striking alteration in the habitual character and pursuits of the individual.
Additional Symptoms.—In some cases there is little appearance of indisposition throughout the day, but the symptoms are aggravated at night; the sleep is uneasy or disturbed by alarming dreams, and in children there is often grinding of the teeth. Pains in the limbs and frequent cramps, general lassitude and muscular debility are often felt, alternating with fits of shivering and feverishness; the digestive functions are disordered; there is a general loss of appetite; often obstinate vomiting; the bowels are either irritable or torpid, the secretions being always unhealthy.
Symptoms Following Inflammation.—The above symptoms precede either general or partial inflammation of the brain. Those which follow indicate more especially the invasion of partial and chronic inflammation, a long-continued, fixed and deep-seated pain in one part of the head; pain, numbness, weakness, a sensation of creeping and tingling in one extremity or in one-half of the body, or confined to one portion of the extremity; there may be numbness and loss of power in one finger only or in one set of muscles. Sometimes the speech is affected so as to produce a degree of hesitation, stuttering or indistinctness of pronunciation, drowsiness, languor, depression of spirits are observed, also more particularly in the chronic form of cerebritis. Some of these premonitory symptoms may have been present for weeks, for months, or even for a year, or for a longer period.
|
|
|
|
|
|
|
General Cerebritis.—General cerebritis is always acute. Its symptoms are divisible into two periods, viz.: 1. The period of irritation or excitement. 2. The period of collapse.
Symptoms.—The symptoms which characterize the period of excitement are intense pain extending over the greater part of the head; great excitement of the cerebral functions; violent dilirium; preternatural acuteness of both the external and internal senses; intolerance of light; brightness, redness, wildness or protrusion of the eyes; contraction of the pupils; tinnitus aurium; flushing of the face; throbbing of the temporal arteries; paroxysms of general convulsion; rigidity of some of the muscles on one or both sides of the body in the interval of the paroxysms. There are also severe shooting pains in the extremities, greatly increased by extending them; twitching of the muscles of the face; rolling of the eyes; quick, suspicious and irregular breathing; rapid, full and hard pulse; subsultus tendinum; red and dry tongue, either tremulous when protruded or in violent motion, pushing out the cheek or forcibly thrust out of the mouth; great thirst; occasionally severe vomiting, especially in children; scanty and high-colored urine. The paroxysms of convulsion are always attended with an exacerbation of the symptoms. The respiration is hurried, and the pulse rises suddenly, forty or fifty beats in a minute. When the convulsions subside the pulse and respiration become comparatively slow and feeble.
Further Symptoms.—The symptoms just enumerated may last from twelve to forty-eight hours or more, when they are succeeded by others of an opposite character, which constitute the second period or that of collapse. The headache is now no longer complained of; delirium gradually passes into stupor or coma; the preternatural acuteness of the senses is succeeded by obtuseness and insensibility; the convulsions subside into general muscular relaxation and more or less complete paralysis succeeds. The pupils become dilated and motionless; the eyes sunk, pale and dim; there is sometimes strabismus or deafness; the pulse is rapid, small, unequal or intermittent; there are frequent rigors, the skin afterward feeling cold and covered with a clammy sweat; the face is pale, sunk and cadaverous; the respiration is slow or irregular and stertorous. When the patient lies senseless on his back and swallows with difficulty, the fatal issue is not far distant. There may be several alternate paroxysms of excitement and collapse until the patient finally sinks into a state of coma, which soon ends in death.
|
|
|
|
|
|
|
Diagnosis.—When the inflammation occupies at the onset a large portion of the brain, it is generally complicated with meningitis and characterized by disturbance in all the vital functions.
Course of the Disease.—When, however, a smaller portion of the brain is engaged in inflammation the course of the disease is seldom so rapid; its invasion is more gradual and preceded by symptoms of irritation in some of the organs of voluntary motion, sensation or intelligence. Convulsive rigidity and retraction of the muscles are sometimes observed in connection with meningitis; but it may be generally distinguished from spasmodic paralysis by several well-marked signs. There is no actual paralysis, and when the convulsive retraction intermits the patient fully recovers the power of voluntary motion in the same manner as after the paroxysms of spasmodic rigidity in tetanus. This convulsive rigidity is scarcely ever limited to one region or to one side of the body as in partial cerebritis, but affects a variety of parts at the same time on both sides.
Treatment.—The inflammatory nature of the more acute forms of cerebritis and arachnitis is so obvious that their treatment has always been conducted in correct principles. Until very lately, however, the inflammatory character of partial and chronic cerebritis was either entirely overlooked or imperfectly understood, that though active treatment was sometimes adopted at the beginning of the disease it was soon laid aside, and remedies of an opposite description substituted. These affections were in fact generally set down as nervous, mistaken for rheumatism, neuralgia, nervous dyspepsia and debility or nervous palsy, and treated by tonics, electricity and stimulants; the fatal termination of the disease being thus accelerated.
Preventive Treatment.—Cerebritis and arachnitis are so formidable that their prevention is of no less, if not greater importance, than their treatment. It is extremely important to have recourse to active measures on the very first appearance of any of the premonitory symptoms, however trifling; as we may thus succeed in effectually removing that state of congestion and irritation of the brain, which is the precursor of inflammation. The means of accomplishing this are the careful and timely removal of all the exciting causes; of every source of irritation, both bodily and mental; regulation of the diet; avoiding all excesses; relaxation from study; change of air; general and local blood letting, counter-irritation, with occasional purgatives.
|
|
|
|
|
|
|
Vigilance Required.—Great vigilance is particularly required in the cerebral affections of infants and children who frequently suffer without complaining. A predisposition to affection of the brain may often be suspected by some slight cost or rolling of the eyes; by dilatation of the pupils, or occasional startings or attacks of spasmodic croupy breathing during sleep; there may be every other appearance of perfect health with these symptoms, which are often only evanescent.
Relieving Congestion.—When it is necessary to relieve the brain from habitual congestion by occasional topical bleeding, the method of taking blood from parts as remote from the disease as possible seems to us preferable to that of abstracting blood from the head itself. When the vessels of a part are partially emptied of their blood, if they have been much weakened by long continued, over-distension or previous disease, so as to have lost their elasticity, there will be an immediate flow of fresh blood to the part; this will take place on mere hydrostatic principles.
Uses of Bleeding.—No fact is better established than that the loss of an exceedingly small quantity of blood from certain parts of the body is sufficient to relieve distressing symptoms of congestion and oppression in others most remote from them; as, for instance, a very slight discharge of blood (one or two ounces) from the hemorrhoidal veins being sufficient instantly to remove vertigo, flushing, headache or oppressed breathing; the same is the case in a still more striking manner with the catamenia, although some account must be taken of the influence of uterine irritation over the system. We prefer, therefore, in cases of habitual congestion in the brain, taking blood occasionally from the feet or legs, by opening a vein or applying leeches and letting them bleed in a foot-bath; or the application of leeches to the arms whenever practicable. We have found this the surest method of affording permanent relief, and by repeating it at certain intervals the tendency to cerebral congestion may be completely overcome. We have pursued this plan in lunatics with the very best results.
Cooling the Head.—The insertion of an issue is often advisible as a preventive in people of a plethoric habit. The head should be kept cool by the frequent use of cold ablutions, the hair cut short, the head and shoulders raised at night; tight bandages round the neck must be avoided; the daily use of the cold shower bath is often very beneficial, but a reaction takes place in the head unless it be used with the feet immersed in hot water. The feet, legs and lower parts of the body ought to be carefully kept warm and dry.
|
|
|
|
|
|
|
Further Treatment.—In the treatment of cerebritis, when fully developed, attention must be paid to its two periods of excitement and collapse. The remedies chiefly to be relied upon are blood letting, general and topical, purgatives, cold applications to the head and counter-irritation.
Treatment of More Acute Cases.—In the more acute cases the patient must be freely bled from a large orifice. If the symptoms continue unabated the bleeding must, however, be repeated several times, at intervals of a few hours, and this practice must be carried during the first period of the disease to the utmost limit of the patient's strength. It often happens that very little impression is made on the disease by the first bleeding and no amendment takes place until after the second. The symptoms often abate after bleeding, but a fresh exacerbation may take place in the course of a few hours. Topical bleeding, by cupping or leeches, is, under such circumstances, highly beneficial.
Head Treatment.—The head must be shaved, and pounded ice mixed with cold water and vinegar may be applied to the scalp. A very effectual method of applying cold is by making the patient hold his head over a basin and pouring a stream of cold water on it from a certain height; this often removes the heat and flushing and calms the excitement; it should be repeated as often as the heat and flushing return. The application of cold to the body is always followed by a reaction, and the temporary relief refrigerants afford will be succeeded by an increase of the inflammatory symptoms and their use become decidedly injurious unless their depressing action be kept up by a steady and repeated application.
Other Remedies.—The remedies next to bleeding and cold, and often not less efficacious, are active purgatives, which must be administered at short intervals until copious evacuations be procured. In some cases no marked amendment has taken place until the bowels have been freely moved; they are sometimes exceedingly torpid, for reasons which have already been assigned, and large doses of cathartics may be required. Combinations of calomel, jalap, scammony, followed by any of the purgative mineral waters, are the purgatives on which the most reliance can be placed. Croton oil is sometimes a valuable remedy, from the facility of its administration and certainty of its effects. Mercury may be given freely as a purgative.
|
|
|
|
|
|
|
Use of an Emetic.—We have sometimes found tartar emetic of great service when there was no irritability of stomach to prevent its being tolerated; the power of tartar emetic in controlling the action of the heart and subsiding the inflammatory diathesis is now fully established; a solution in the proportion of one grain to the ounce and a tablespoonful given every hour or two, suspending it should vomiting occur, has often been attended with great benefit. The remedy is in general well tolerated, owing to the torpor of the stomach; violent vomiting should, however, be prevented, as it would obviously be extremely injurious.
Treatment of Second Stages.—In the second stage of acute cerebritis, that of collapse and coma, general blood letting is to be used most sparingly; decided advantage, however, has resulted from a moderate bleeding even at a late period. In this stage topical bleeding is more generally indicated. There are periods of exacerbation in the symptoms which should be watched and overcome by these means, which may be persevered in as long as there is any hardness and resistance in the pulse. We have seen a patient instantly recover from a state of profound coma by the abstraction of a very small quantity of blood with the cupping glass. In this stage we may have recourse to counter-irritation with advantage; blisters may be applied between the shoulders, to the occiput or to the neck or legs. There is an objection to their being applied to the whole head, that it prevents the subsequent application of cold. We have, however, in desperate cases, seen a decided amendment follow the application of a large cap blister. Particular attention should be paid to the abdominal region, and especially that of the bladder, which ought to be examined morning and evening in order to detect retention of urine, and we must take care not to be led into error by an incontinence of urine from the over-distension of the bladder; this must be obviated by drawing off the urine with the catheter twice a day.
Treatment of Chronic Forms.—In the more chronic forms of cerebritis, unattended with fever or much general excitement, the same activity of treatment is of course not admissible. We must still, however, pursue the antiphlogistic plan, modifying it according to the urgency of the symptoms. During the period of irritation, with cephalalgia, vertigo, or rigid spasm of the extremities, moderate bleeding, general and topical, purgatives and counter-irritation are the only remedies from which any advantage is to be expected; they must be repeated at longer or shorter intervals, according as the strength of the patient and the continuance of the symptoms may seem to indicate. A great deal is to be accomplished in all chronic inflammations by persevering in a moderate course of antiphlogistic treatment. We must watch, carefully any signs of amendment, remembering that there is a great tendency to collapse, and that the natural course of the complaint is characterized by irregular remissions and exacerbations.
|
|
|
|
|
|
|
When to Cease Active Treatment.—When the period of irritation is over, and is followed by a remission of all signs of excitement, by a complete paralysis of the muscles, and by other evident signs belonging to the period of softening and suppuration, the strength of the patient must no longer be reduced by active treatment. In all inflammatory diseases, when the stage of excitement and disorganization is over, a process of reparation commences, which requires for its completion a certain degree of power in the constitution. If at this period we persevere in lowering the general strength, we deprive the constitution of its natural resources and interfere with its healing operations.
When the Excitement Turns.—It becomes, therefore, an object of considerable importance to watch the moment when the tide of excitement is on the turn, and when the powers of the constitution are verging to a state of collapse, in order that we may abstain from an injurious interference, husband the patient's strength and even support it if required. This precaution is particularly necessary in old people and young children.
Convalescence.—After convalescence has been established the patient will still require to be closely watched for some time before his recovery can be considered fully confirmed; he must be kept perfectly quiet, free from every species of excitement and the regimen duly regulated. When the brain has once suffered from inflammation it is slow in recovering its tone, and the most trifling cause, such as a slight mental exertion or emotion, a full meal, and so forth, has been in many cases sufficient to occasion a relapse.
Suppressed Menstruation.—When cerebritis has occurred after suppressed evacuations or the metastasis of other diseases, we should endeavor to procure their return. If menstruation is suppressed, leeches should be applied to the pubis or inguinal regions, and the frequent use of hot pediluvia recommended. If cutaneous eruptions or rheumatic gouty pains in the joints previously existed, blisters or rubefacients are to be applied to the parts originally affected.
Summary of Symptoms of Brain Congestion.—The following summary gives a connected view of the various morbid conditions of the brain, which are the effects of congestion and inflammation, together with their symptoms:
Cerebral Congestion.—Cerebral congestion, over-distension of vessels; vertigo, tinnitus aurium, confusion of sight, cephalalgia, if the pressure in the vessels be carried to a sufficient extent to intercept the circulation; simple apoplexy, seldom fatal, recovery rapid.
|
|
|
|
|
|
|
Permanent Cerebral Congestion.—If the cerebral congestion be permanent, or returns frequently; drowsiness, oppressed intellect; the vessels become weakened and on a sudden increase of congestion are ruptured; extravasation of blood, sanguineous apoplexy; destruction of cerebral substance and compression; loss of consciousness, permanent or temporary; sudden and complete paralysis without spasmodic affection of the muscles.
General Congestion.—General congestion, followed by inflammation of a considerable portion of the brain; deep injection; partial sanguineous infiltration; dotted and ecchymosed striated appearance of the cerebral substance; general cerebritis (combined usually with arachnitis). Period of high excitement of all the cerebral functions, with general convulsions, followed by a period of collapse and coma.
Partial Congestion.—Partial congestion and inflammation of the brain; 1st period, the same deep injection and sanguineous infiltration, more circumscribed; partial cerebritis. Partial symptoms of irritation in the organs of motion and sense; weakness, pain, numbness, spasmodic paralysis, confined to one side or a few regions of the body. 2d period, infiltration of pus in the cerebral substance; softening; abscess; complete paralysis; relaxation and flaccidity of the muscles; loss of feeling; abolition of some of the external senses or intellectual faculties; death, either gradual or sudden, by the extension of the inflammation or by pressure.
Cerebral Inflammation.—After sanguineous apoplexy and sudden and complete paralysis, inflammation of the cerebral substance surrounding the coagulum; consecutive cerebritis, the paralyzed limbs affected with pains, convulsive motion, spasmodic rigidity.
Slow Congestion.—Slow and gradual congestion with very slight irritation; long, continued state of low inflammation, ending sometimes in softening, sometimes in induration, or else in an infiltration of serous fluids and white softening. Various forms of chronic cerebritis, sense and motion very gradually weakened and impaired without pains or spasmodic rigidity in the muscles.
(Hydrocephalus.)
Causes.—Water in the head; dropsy of the brain. This is almost always an affection of early life. Sometimes it is congenital. It is mostly a passive dropsical effusion; certain cases show signs of a chronic or subacute inflammatory condition of the arachnoid membrane of the brain,
|
|
|
|
|
|
|
Symptoms.—Languor, strabismus, convulsions, loss of appetite and increase in the size of the head. This last may be enormous.
Treatment.—Moderate purging every few days, or once a week, sustaining the strength by nourishing food, and, if it be borne, cod-liver oil; diuretics; shaving the head and rubbing it nightly with mercurial ointment; occasionally blistering the back of the neck, in a child. Pneumatic aspiration may perhaps prove useful in hydrocephalus. To remove the fluid gradually and safely mild stimulating baths have a very beneficial influence.
Symptoms.—The symptoms of this uncommon affection are: constant and severe pain in the back increased by motion; spasmodic contractions or rigidity of the muscles followed by paralysis, fever, constipation of the bowels and retention of urine. In myelitis proper, as distinguished from spinal arachnitis, there is no pain or muscular rigidity but only paralysis of motion and sensation.
Treatment.—Cupping or leeching along the spine, followed by a blister and active purgation with saline cathartics, constitute the essential parts of the treatment of simple inflammation of the spinal cord or of its membranes.
Causes.—These have been divided into external or obvious and internal or such as can only be discovered after death. The external causes or those acting mechanically by evoking pressure on the brain; such are fracture of the skull with depression of a portion of bone, or blood extravasated immediately beneath the fractured bone without depression. The reality of this cause is shown by the effect of direct pressure made upon the surface of the brain by the point of the finger in cases where a portion of the skull has been removed by the trepan, or on the fontanelle or opening between the cranial bones in the head of infants. Causes tending to increase the arterial action of the brain, either by direct application to the head itself, or indirectly through the medium of other organs. Causes which operate by impeding the return of blood from the brain, as stooping; the application of a tight ligature round the neck so as to compress the internal jugular veins; tumors of any kind so situated in the neck or chest as to interrupt the return of blood from the brain to the heart; diseases of the heart or lungs impeding the transmission of the blood through the pulmonary vessels; or a voluntary suspension of breathing after a full inspiration; or in blowing wind instruments, or in making great muscular efforts of any kind. The internal causes are those that are only discoverable after death, viz., extravasation of blood in the substance of the brain or in the ventricles, or serous accumulations in any of the cavities or between its membranes.
|
|
|
|
|
|
|
Symptoms.—We have two forms of genuine apoplectic seizure: congestive and hemorrhagic. In the first the premonitory symptoms are, flushed appearance of the face and eyes, heat of head, throbbing of the carotids, distension of the temporal arteries and jugular veins; constipation, languor, dullness, drowsiness, dimness of sight, vertigo, headache. The attack is marked by sudden stupor; with slow and sometimes snoring respiration, full and slow pulse, dusky or turgid appearance of the face. The total loss of perception may be brief, its partial absence or deficiency continuing for some time. Slight convulsive movements are not uncommon. Paralysis of the muscles occurs only for a short time after the attack, if recovered from.
Hemorrhagic Apoplexy.—In hemorrhagic apoplexy generally no clear premonition is given, the attack being very sudden; a stroke, literally unconsciousness is complete for some seconds, minutes or hours. After this, general or local paralysis, most often hemiplegia (paralysis of one side of the body) is left; the mental powers also, in many cases, being impaired at least temporarily, during the coma; the breathing is commonly stertorous and the pulse slow and somewhat full, the head hot and the face more or less dark or flushed. But the fullness of the blood-vessels and heat of the head are much less, as a rule, than in congestive apoplexy.
The younger the patient and the more vigorous his antecedent health the more probable is the existence of the congestive form; and, also, the better the prospect of recovery from hemorrhage within the cranium, if only the effects of pressure be exerted at the time.
Treatment 1.—If, in a person under fifty, not before of broken constitution, we find the head hot, face turgid and flushed, the arteries and veins of the neck and temples full, the pulse also strong, and the heart's impulse so (or the heart's action vigorous though the pulse at the wrist be oppressed) blood may be taken, carefully, from the arm or by cups ox leeches applied to the back of the neck.
2. Older and more doubtful cases may be treated tentatively with cups alone, aided by mustard plasters to the legs, back and epigastrium in turn; with laxative injections into the rectum during the attack and saline purgatives afterward. The head should be kept raised and cooled with wet cloths until its temperature becomes normal. If the hair be thick, it should be cut very short or shaved off entirely and an ice-cap placed thereon over the whole surface. When, however, there is reason, as usually is the case in really old or broken-down patients, to believe the structural degeneration, arterial or that of ramollissement, is the source of the attack, loss of blood will be out of place.
|
|
|
|
|
|
|
Symptoms.—Loss of speech may occur as one of the symptoms of disease of the brain, either functional and transient, or organic and irremovable. Such a loss of language is termed aphasia, not articulation, as in aphonia, but expression is, in this affection, wanting. The power to unite words from memory, to convey meaning, is lost; but, in some cases, at least, they may be copied correctly.
Causes.—Hemiplegia of the right side has in a number of examples coincided with aphasia, and, several times, also, autopsy has shown softening or other lesion of the left anterior portion of the cerebrum. Valvular lesion of the heart sometimes accompanies this disease.
Treatment.—Cases of aphasia are very rare. There is no special measure of treatment except that of general principles, and treat untoward ones as they arise.
Symptoms.—This is a disease occurring in persons exposed to excessive heat and characterized by vertigo, sometimes with violent pain in the head, gradual increase of listlessness and torpidity and a desire to lie down. The feverish symptoms may culminate in more or less sudden and complete insensibility.
Treatment.—The most obvious demand in regard to treatment is to abstract the excessive heat from the body as rapidly as possible, and this can be most speedily accomplished by cold sponging, rubbing the head, neck and chest with ice or by the cold pack. Light should be excluded from the patient as far as possible, and if the pulse is feeble stimulants should be given by the mouth or by injection. If prompt improvement does not occur the hair should be cut short and a blister applied to the nape of the neck.
|
|
|
|
|
|
|
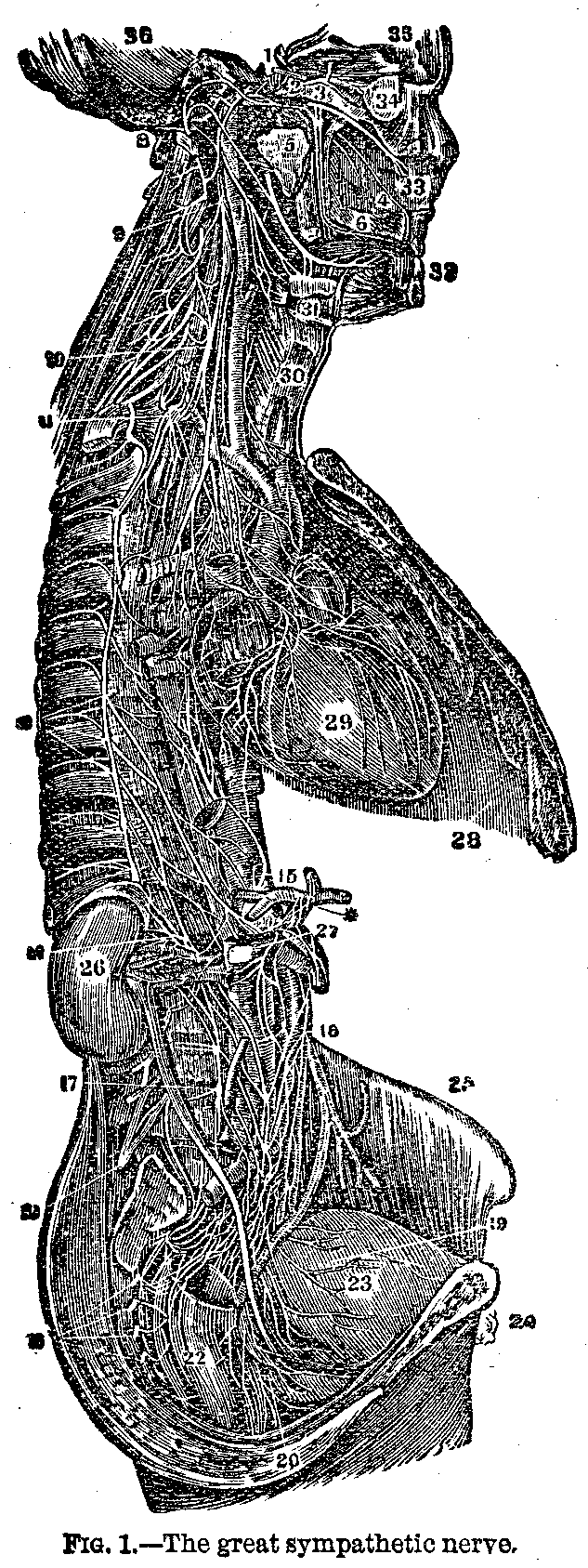
FIGURE NO. 1.
1. Plexus or bunch of nerves in the carotid region.
2. Sixth external motor nerve.
3. First branch of the 5th ophthalmic nerve.
4. A branch on the nose partition, which goes to the incisive foramen.
5. Concurrent branch of the Vidian nerve, dividing itself into carotid
and petrosas branches.
6. Back branches of the palate.
7. Lingual nerve joined by the tympanum cord.
8. Hard part of the 7th pair or facial nerve.
9. Upper cervical ganglions.
10. Middle cervical ganglions.
11. Lower cervical ganglions.
12. Roots of the great splenic nerve.
13. Lesser splenic nerve.
14. Renal plexus.
15. Solar plexus.
16. Mesenteric plexus.
17. Lumbar ganglions.
18. Sacrum ganglions.
19. Vesical plexus. /
20. Rectum plexus.
21. Lumbar plexus.
22. The rectum.
23. The bladder.
24. The pubis.
25. Crest of the ileum.
26. The kidney.
27. The aorta.
28. The diaphragm.
29. The heart.
30. The larynx.
31. The submaxillar gland.
32. The incisive teeth.
33. The nasal partition.
34. Globe of the eye.
35, 36. Cavity of the cranium.
FIGURE NO. 2.
1. Section of the bone of the forehead.
2. Section of the occipital bone.
3. Muscles in the back of the neck.
4. Integuments on the skin.
5. Frontal cavity.
6. Middle spongy bone.
7. Lower spongy bone.
8. Middle passage of the nose.
9. Lower passage of the nose.
10. Thickness of the roof of the mouth and depth of the nose.
11. Opening of the eustachian tube. The catheter is at the nose and
is going through the tube.
12. Cartilage of the nasal division.
13. Genio-gloso muscle.
14. Veil of the palate.
FIGURE NO. 4. 1,1. The cubital nerve. 2,2. The ramus profundis dorsalis (deep-seated nerve of back of arm). 3. Extreme of the cutaneous nerve of the arm. 4. Branch of the radial nerve. 5,5. Back view of the digital nerves, o of the fingers. 6. Back branch of the cubital nerve
|
|
|
|
|
|
|
For an explanation of the illustrations see text on opposite page.

|
|
|
|
|
|
|
Heat Exhaustion.—In heat exhaustion the patient is generally found with a cool skin, a feeble pulse and pallid face, without disturbance of the intellect. In such a condition stimulants, dry heat of hot-water bags or bottles, mustard plasters to the stomach and perfect rest and quiet are indicated.
Meaning.—Hypertrophy means an actual enlargement or overgrowth of the brain structure generally, while atrophy signifies a general wasting of the substance of the brain.
Causes.—The brain is sometimes the seat of morbid growths, including cancers, fibroid and bony tumors, tubercular deposit in large masses, and casts containing parasites. All these affections are, fortunately, very seldom met with.
Treatment.—The treatment in such cases is, of course, to cut out the tumor and the affected portion of the nerve with as little delay as possible, whenever it can be accomplished.
Causes.—Palsy is one of the most common and most distressing misfortunes from which mankind is obliged to suffer. Yet its various forms are rather symptoms of deep-seated disease than disease themselves. Thus palsy of a limb is very frequently a symptom of structural disease of the brain or spinal cord, but it occasionally occurs from a diseased nerve trunk itself. It may affect a whole limb or only part of one, and is sometimes limited to a group of muscles in a particular region.
Symptoms.—The following conditions give rise to paralysis of motion:
1. Disease or injury to a nerve in some part of its course, destroying its power of transmitting the force, which is expressed by a contraction of the muscle to which the nerve is distributed.
2. A disease of some portion of those central parts of the nervous system, whence the nerve takes it origin, or with which it may be connected directly or indirectly.
Varieties of Palsy.—There are many varieties of palsy, among the most important of which are the following:
According to its nature it may be motor (acinesia), and sensory paralysis (anesthesia).
Facial Palsy.—This is an affection of the portio dura of the seventh pair of cephalic nerves, the motor nerve of the face. It occurs at any age, usually from rheumatoid inflammation of the sheath of the nerve at its escape through the cranium, through the stylo-mastoid foramen.
|
|
|
|
|
|
|
Symptoms.—On one side of the face is without change of expression, and the eye on that side is not closed (in severe cases) from the paralysis effecting the orbicularis palpebra muscle. The tongue is not affected in the movements. The facial motor nerve is not often involved in the much more serious cases of cerebral palsy.
Diagnosis.—Absence of disturbance or of incompleteness of control over the tongue, while the power over the eyelid is partly or wholly lost with the absence of severe cerebral symptoms, will, especially in a young person, make the diagnosis easy as well as important.
Treatment.—The treatment of this form of local palsy may be by repeated small blisters behind the ear, followed, when convalescence has begun, by some warm covering (cotton wadding, flannel or silk) to protect the part from cold.
Writer's Cramp.—Pressure upon a nerve may cause its paralysis, generally temporary. A man has been known to have his hand rendered powerless for three weeks by sleeping all night with his arm bent under his head. Friction, the endermic application of strychnia and galvanism may be used in such a case. Writer's cramp or scrivener's palsy, is the result of exhaustion of certain muscles from over-use. Its cure is rest.
Hemiplegia.—This means half palsy and is a paralysis in which one lateral half or side of the body is stricken with powerlessness so accurately that it is customary to define the condition by the terms right and left.
Causes.—Brain lesion is most often the cause of this affection; either an apoplectic clot, a tumor or softening.
Symptoms.—In severe cases the arm and leg may be equally motionless, but if there is any difference between them the leg is generally the limb less affected, the last to be attacked, and the first to recover some of its powers. Suddenly, almost always, but not always with loss of consciousness, the patient loses the power of motion and more or less sensation on one side. In complete cases the parts involved are the arm and leg, the muscles of mastication and half of the tongue.
Treatment 1.—Essentially the same principles are applicable to this as have been mentioned in connection with apoplexy. The younger the patient the more vigorous his or her previous health, and the fuller the circulation the more appropriate may be the general or local abstraction of blood to diminish pressure upon the brain. Where softening is apprehended bleeding should be exceptional and cautious. Rest, regulation of the bowels, and counter-irritation of dry cups to the upper part of the spine, and afterward a blister, with friction, as with brandy and red pepper, or whiskey and hot water, or salt and spirits, to the affected limbs.
|
|
|
|
|
|
|
2. In the hysterical form, if it lasts long, electricity may be applied locally with safety and advantage. In any curable case passive exercise of the weak limbs will be very useful.
Paraplegia.—Paraplegia is that form of palsy in which one-half of the body below the chest and including the lower limbs is stricken with the disease.
Causes.—Spinal disease or injury is its source, with or without cerebral implication or complication. It may come suddenly or gradually, generally its beginning, at least, is sudden.
Symptoms.—When the spine is affected, as well as in the reflex form, numbness in the feet and pain in the back are apt to be early signs. The power of motion is lessened or lost in the lower limbs. The muscles may be either relaxed or contracted. The lesion of the spinal marrow, if progressive, is productive of loss of power over the bladder and bowels. Bed-sores with deep ulceration and sloughing may occur in protracted cases.
Treatment.—When myelitis is believed to exist, at an early stage, local depletion to a moderate extent may be advised. In may cases counter-irritation by repeated sinapisms, or stimulating liniments will be proper. While inflammation or active irritation of the spinal cord is made apparent by the symptoms (pain, cramps, muscular twitching or rigidity), strychnia is not suitable. After these have subsided it may be given, not more at first than the thirtieth of a grain twice daily. If it produce jerking movements of the hands or feet, or nervous restlessness, or any marked uneasiness it should be suspended. Electricity may be used with similar caution in a secondary stage of paraplegia.
Hysterical Paralysis.—In females this is among the many forms of functional disorder which that strange but not yet clearly defined disorder, hysteria, may produce.
Diagnosis.—The affected limb, in walking, is dragged after the other, as if a dead weight; while in cerebral hemiplegia the palsied leg and foot are brought round in a curve, the body being bent toward the sound side at the time.
Treatment.—-Tonics, good nourishment and change of air are most required in all hysterical cases. For the paralysis itself electricity is useful. Mild shocks for a few minutes twice a day may be given with advantage.
|
|
|
|
|
|
|
Reflex Paralysis.—Causes.—Worms, dysentery, diarrhoea, uterine irritation, teething and external injuries are all thought, to induce reflex paralysis in certain instances. Diphtheritic and scarlatinal palsies have been placed in the same category. The simplest and clearest cases are those of wounds.
Treatment.—In true reflex paralysis the removal of the irritant cause produces instant relief. When the nature of the case does not admit of such prompt relief, if the diagnosis be clear, the same indication remains, to address our remedial measures to the seat or source of peripheral irritation. Palliate, if we cannot cure the trouble there, and we will obtain palliation, if not relief, of the reflex disability. Electricity has proved signally useful in the subsequent treatment.
Diphtheritic Paralysis.—After the termination of an attack of diphtheria, commonly within three weeks, the muscles used in swallowing and speaking, less often those of the upper and lower limbs and the sense of sight may be partially paralyzed. Loss of sensibility usually accompanies the loss of motor power. This condition of things may last for weeks or even months, but is generally recovered from.
Causes.—The immediate cause of the paralysis of the peripheral lesion of the nervous terminations is the toxemic influence upon those centres of the morbid poison of diphtheria.
Treatment.—Passive exercise, stimulating friction and electricity, change of air and sea-bathing are suitable measures for this affection.
Syphilitic Paralysis.—The most unequivocal instances of this nature are accounted for by periostitis within the cranium, involving the dura mater, or by nodular exostosis pressing upon the brain. The most remarkable fact connected with such cases is the prompt curative effect upon it of iodide of potassium.
Lead Palsy.—Considerable time of exposure to the influence of lead is generally necessary to cause this. So commonly does it first affect the extensor muscles of the forearm that the cognomen of "wrist drop" is often applied to it. When it lasts for some weeks the muscles waste away.
Symptoms.—A blue line is observed to form along the edge of the gums. Pain precedes the palsy and attends recovery of power. Mostly, though after a long time, lead palsy is recovered from.
Treatment.—Iodide of potassium appears to act as an eliminant of the lead accumulated in the system. Ergot is also useful. Faradaic electricity has been found decidedly beneficial used in moderate strength for a few minutes two or three times a day.
|
|
|
|
|
|
|
Mercurial Palsy.—This is occasionally met with in those who work in metal. Mostly tremor is a predominant symptom. Early withdrawal from the influence of the cause and the continued use of the iodide of potassium are the principal measures of treatment.
Paralysis Agitans, called also shaking palsy, is described as a more or less constant involuntary and uncontrollable shaking of the hands, arms; head or, progressively, of the whole body. Slight or moderate degrees of such tremor are common enough from general nervous debility. Extreme cases evince the wreck of the cerebro-spinal system and are, therefore, incurable. In other cases the treatment is upon general principles.
Progressive Muscular Atrophy.—This is still another uncommon and incurable form of paralysis due to a gradual decay and wasting of the muscles, but commencing sometimes with an apparent enlargement or hypertrophy of these organs.
Locomotor Ataxia.—This results from a disease called sclerosis, or hardening of certain motor-centres in the brain and spinal cord.
Symptoms.—Rheumatoid pains precede loss of power, occasional strabismus (cross-eye) and incontinence of urine may occur. Then there is an awkward, unsteady gait; the sensibility of the feet becomes blunted, and walking is insecure. If the patient shuts his eyes he falls down, and even with them open he reels as if drunk. The duration of this progressive disease varies from six months to ten or twenty years.
Treatment.—Hygienic management, general tonics, electricity and very careful use of strychnia.
Infantile Paralysis.—This is a variety developed in very young children and occasionally present from time of birth. As a rule this palsy arises from disease of the spinal cord and its membranes.
Symptoms.—It comes on with acute symptoms of fever and convulsions, ending in paralysis of one or more limbs. In some cases the child gradually recovers from the effects of the malady, but in many the impairment is permanent and the limb, ceasing to develop in proportion to the rest of the body, appears in the adult as if shrunken and withered, constituting a lamentable and hopeless deformity.
Treatment.—Much can be done towards preventing complete loss of power by persevering and systematic movements, application of galvanism and exercise as suggested in the article on hemiplegia.
Scrivener's Palsy.—Called also writer's cramp. It is the result of long continued and unnatural excitement of the nerves controlling the fingers and hand in writing.
|
|
|
|
|
|
|
Symptoms.—The earliest indication is a painful sense of fatigue and weakness which come on shortly after commencing to write. Sooner or later this begins to be accompanied by involuntary spasms of the muscles employed in holding the pen and the handwriting grows unsteady, scrawly and almost illegible. At first the spasms and irregular movements can be more or less controlled by voluntary effort but they gradually become worse and worse, until at last the use of the pen is an impossibility.
Treatment.—Rest from writing, tonics and electricity accomplish a cure in some instances, but the prospect of recovery is small, and it is, therefore, very important to avoid the disease by moderation in writing, or by the use of the ingenious typewriter.
Wasting Palsy.—A few of the muscles of one limb, or the voluntary muscles of the whole body may lose their power and then waste away to almost nothing. Insidious in its approach the affection may last from six months to several years. It may end in recovery. The shoulder and ball of the thumb are frequent points of commencement for the palsy and atrophy.
Description.—When a patient is the subject of an uncontrollable spasmodic contraction of the muscles of the lower jaw, he is said to have "trismus" or lock-jaw; and when the same condition attacks other or all the voluntary muscles of the body he is said to have "tetanus."
Causes 1.—Tetanus includes trismus and generally begins with it, though trismus may be a local affection. It is found in children as a result of dentition, and in adults as a consequence of diseases involving the teeth, gums or jaws. It is a spasmodic affection produced by reflected irritation set up by a local disease, is rarely associated with any constitutional disturbance and is, for the most part, cured on removal of the cause.
2. Tetanus is likewise generally associated with some local source of irritation, some wound or injury, it is then called "traumatic;" when an external or visible cause can be made out, it is denominated "idiopathic;" when rapid in its course it is called acute; when slow, chronic. The acute form is usually the result of an accident and generally fatal. The chronic is for the most part idiopathic and more curable.
Symptoms.—There are no general or local premonitory symptoms by which the onset of this affection can be recognized, and the earliest indications of its approach are generally a difficulty in opening the mouth, with stiffness in the muscles of the lower jaw; yet these symptoms may be so slight as to pass unheeded, or to be misinterpreted, when, however, some rigidity of the muscles of the neck, throat or abdomen can be made out and the first indications of the "tetanic grin" recognized.
|
|
|
|
|
|
|
3. As the disease progresses the muscular system of the body generally will be more or less affected, and, in different cases, different groups of muscles will be involved. Those of the back are most frequently attacked and their contraction may be so powerful as to cause an arching backward of the frame. The muscles of respiration are, as a rule, affected only in acute cases, and the chief danger to life consists in the severity of the spasms which attack them. When severe the first spasm may be fatal and may occur at an early or at a remote period of the affection. When the jaw is unlocked by a spasm of the depressor muscles, the tongue is sometimes suddenly shot out from between the teeth and often wounded.
4. As the disease advances the jaws become completely fixed and deglution is then impossible. The spasms of the muscles of the frame become more intense and frequent and the powers of the patient rapidly decline. The pulse which was rapid becomes more feeble, while the expression of the countenance betokens agony of the body and despair of the mind. The slightest manipulation or movement of the patient sets up a fresh spasm, and any emotion may do the same. The skin becomes bathed with a cold sweat, and, if death is not caused by suffocation, exhaustion soon puts an end to suffering.
Treatment.—Among the specific remedies which have been greatly trusted the Colabar bean stands foremost and may be given in full doses, such as half a grain of the extract in two or three hours. Camphor is also recommended in doses of from five to ten grains. The bromide of ammonium or potassium has been administered with advantage. It was hoped that a valuable drug for this disease had been found in chloroform, but experience has not justified the expectation. The hydrate of chloral has now taken its place and been of some service. Indian hemp in doses of a grain every hour, aconite and belladonna in quantities of one-fourth of a grain have also been recommended. Ice applied in bags along the spine has apparently been of great value. The administration of remedies by subcutaneous injection, in these cases, promises to be a valuable adjunct to practice, enabling us rapidly to introduce into the system drugs which act antagonistically to tetanic spasm.
|
|
|
|
|
|
|
Meaning the "dread of water," which is more correctly termed "rabies" is a disease contracted from a rabid animal, generally from its bite through the saliva or mucus.
Stages of the Disease.—In the dog there are three well-marked stages of the complaint. The first is the melancholic, characterized by melancholy, depression, sullenness and fidgetiness; the second, the furious, by excitement or rabid fury, and the last, the paralytic, by general muscular debility and actual paralysis.
Symptoms 1.—In man the disease may show itself at any period from six weeks to a year after the inoculation. A month or more after the bite of a mad dog, or other rabid animal, the wound having healed, irritation is felt in it, nervous restlessness also exists which increases (in most cases) to violent, angry delirium. Then difficulty of swallowing occurs from a spasm of the muscles of inspiration (gasping) taking place at the moment of deglutition, making the patient choke.
2. The same spasmodic gasping is brought on by any sudden impression, as of sound, a flash of light or even a current of air passing over the face. Insomnia exists; the patient grows prostrate and must die for want of food and drink, even if the affection of the cerebro-spinal axis were not itself fatal.
3. There is intense thirst, but the characteristic dread of water, not as a fluid, however, but as connected with the difficulty of drinking. The sight of water is frequently sufficient to bring on shuddering, yet it is when the patient carries water to his lips that he is seized with the typical terrors.
4. A rabid man is always rational and tries to drink but the attempt excites terror and the expression of his inability. His eyes become fixed, features contracted and his countenance expressive of the deepest anxiety, his limbs shake, and the whole body shivers. The paroxysm lasts a few seconds, then subsides, but only to be renewed on the slightest breath of air touching the body. During the calm sudden terror of an unknown kind haunts the mind and imaginary calling of friends often exists.
Symptoms of Last Stage.—In the third and last stage the longing for drink becomes intense, with an increasing inability to take it; the voice becomes hoarse and the mouth full of frothy fluid. The patient tries to get rid of this by spitting, and then becomes frightened at its results. Convulsive seizures increase in frequency and intensity, the spasm of the respiratory muscles threatening life; at last a fatal spasm takes place and death by asphyxia ensues.
|
|
|
|
|
|
|
Treatment.—There is not satisfactory evidence that a case of genuine rabies canina or hydrophobia has ever been cured. If we cannot cure, what can or should we do? We may certainly promote easy death by allaying the wretched sufferings of the patient by nitrous oxide, ether, or chloroform. Hypodermic injection of atropia or morphia might, perhaps, more effectually quiet the suffering and even afford more possibility of cure than inhalation of anesthetics. In all cases of bites from dogs or animals, however, in which the faintest suspicion of rabies exists, free cauterization with lunar caustic should be performed. Mental stimulants, in the way of inspiring hope and removing fear, must be duly administered and such general treatment as may be needed. No drug has yet been discovered that has the least influence on the disease, either in preventing or curing it.
What is known as the "Pasteur cure for hydrophobia" is in great favor among some medical men. It is rather a preventive agent or treatment and no doubt possesses great value.
Causes.—The exciting causes are numerous, constipation of the bowels, indigestion, worms, irritation of the gums in teething and excitement of the brain, as by fright, are about the most frequent. Many acute and chronic diseases of infancy (scarlet fever, meningitis, whooping-cough, and so forth) have convulsions among their occasional symptoms or complications.
Symptoms.—Premonition of a fit is often observed in the child's fretfulness, or restlessness, or gritting of the teeth in sleep. When a fit comes on the muscles of the face twitch, the body becomes rigid at first, then in a state of twitching motion, the head and neck are drawn backward, the limbs violently flexed and extended; sometimes these movements are confined to certain muscles, or are limited to one side.
Treatment 1.—The treatment of a child during the convulsion is, of course, to be directed first toward relaxing the spasm, and immediately after that is accomplished to removing the cause of the trouble, which, in two cases out of three, will prove to be irritation of the gums or bowels. To shorten the paroxysm the child should at once be placed in a warm bath and a cloth wrung out of cold water applied to its head.
2. If the gums are swollen, or have been tender and irritated at the time of teething, lance them freely, dividing the tense gum down to the coming tooth. If the bowels have not been moved give at once an enema of castor oil, soap and molasses, or some other laxative material, with warm water. If there is reason to suppose that the intestinal worms, which most children harbor, are causing disturbance, active vermifuges such as a grain of santonine before dinner and supper for a child two years old, followed by two grains of calomel at bed-time, ought to be employed.
|
|
|
|
|
|
|
3. Cupping the back of the neck, in some cases where time is allowed by a protracted fit, may be resorted to, especially dry cups. Full doses of bromide of potassium, asafetida and valerian are often very useful in diminishing the excitability of the nervous system, which is especially great during the age of childhood.
Prescription:
Rx.---Bromide of ammonia...................... 40 grains
Bromide of potash....................... 1/2 drachm
Fluid extract of gelsemium.............. 20 minims
Extract of valerian fluid............... 20 "
Water ................................... 1 ounce
Half a teaspoonful for a child 2 years old, every
2 or 3 hours.
Periodical convulsions with unconsciousness during the attack.
Causes.—Hereditary transmission of this disease is common. Intemperance, venereal excess and self-abuse, blows on the head and fright are among the most frequent exciting causes.
Symptoms.—Premonition occurs in a minority of cases before an attack; headache, dizziness, terror, spectral illusions, a creeping or blowing sensation, like that of a current of air or stream of water, beginning in a hand or foot and extending toward the trunk. Then, often with a scream, the patient falls down and is violently convulsed. Foaming at the mouth, grinding of the teeth and biting of the tongue are common; the face is flushed, the eyeballs roll, the pupils are unaffected by light, sometimes vomiting, or involuntary urination or defecation takes place; the respiration may be very laborious. The fit lasts on an average from five to ten minutes. The interval between the attacks may be from several months down to a few days. In old cases there may be two or three paroxysms daily. They vary much, even in the same individual. The condition after the attack is also various, generally drowsiness or deep sleep follows it, or headache, debility or delirium, sometimes maniacal frenzy.
|
|
|
|
|
|
|
Treatment 1.—During the paroxysm, when habitual, little can be done. Place the patient so that he cannot strike his head or limbs against any thing hard, loosen the clothing about the neck to form free respiration and circulation and insure fresh air about the patient, protect the tongue from being bitten, if possible, by placing a cork or piece of India rubber between the teeth. Care must be taken that such an object does not pass into the throat and choke the patient, which can be prevented by trying a strong string to it.
2. To break up the recurrence of the fits is the problem for which a vast number of remedies have been tried in vain. Bromide of potash, valerianate of zinc, belladonna, arsenic and digitalis have all been employed. Strangely enough this disease is very apt to improve temporarily under any new treatment, no matter how absurd, which takes a strong hold on the patient's imagination.
3. Self-management is very important to the epileptic. Temperance with nutritious diet is necessary; regularity of the evacuation of the bowels is imperative; abundant exercise in the open air, short of exhaustion, does good; systematic gymnastics have even cured some cases.
PRESCRIPTION.
Rx.---Bromide of potash....................... 3 drachms
Bromide of soda......................... 3 "
Bromide of ammonia...................... 3 "
Iodide of potash........................ 1-1/2 "
Iodide of ammonia....................... 1-1/2 "
Carbonate of ammonia.................... 1 drachm
Tincture of columbae ................... 1-1/2 ounces
Water .................................. 6-1/2 "
Take two teaspoonfula before each meal and three
teaspoonfuls at bed-time.
Causes.—This is the most important of several varieties of simple spasm in different parts of the body. Among which ordinary croup is a familiar example. It consists in a spasm of the muscles of the glottis or opening into the windpipe, by which a crowing or croupy cough is produced, with hard or stridulous breathing.
Symptoms.—This disease especially occurs in young children, where it is due to some reflex irritation, such as that of teething, reflected from the nerve centres which control the muscles of the glottis. It may generally be distinguished from the alarming malady, true croup, by its coming on suddenly without fever, marked heat of skin or quickened pulse.
|
|
|
|
|
|
|
Treatment.—To relax the spasm sprinkling of a little cold water in the face, or tickling the fauces with the finger or with a feather, so as to produce vomiting frequently answers the purpose. Should it fail the child should be immediately placed in a warm bath. After an attack the gums should be carefully examined and freely lanced if found swollen, every attention being paid to the general health. Much needless alarm would be spared to anxious parents and nurses if it were generally understood that there is no likelihood of this disease leading on to the fatal malady, true croup, which may always be excluded from consideration if the child is free from fever, coughs loudly and has no huskiness of the voice.
Causes.—From six to sixteen, in both sexes, especially often, however, in girls, chorea occurs. Nervous debility is almost always present before the attack. Fright is a frequent cause, overfatigue or mental excitement, blows or falls may produce it. Rheumatic fever is sometimes followed by it.
Symptoms.—Incessant and irregular movements of the voluntary muscles over which the will has but partial control. Walking in severe cases is difficult or unsafe; the hands cannot be regulated enough to write or work; speech may be affected; the muscles of the face often twitch grotesquely. The pupil is, in some cases, unnaturally dilated; palpitation of the heart may occur, and also constipation and indigestion. The urine is of great density; the countenance assumes a blank and foolish expression, and the mind itself may in time grow seriously enfeebled.
Treatment.—Good diet, salt bathing and systematic gymnastic exercises will suffice for mild cases. Where marked anemia exists iron (citrate, phosphate or hypophosphate, tincture of chloride, syrup of iodide) is important. Obstinate cases may be treated with Fowler's solution of arsenic, in small doses, gradually increased. Cod-liver oil should be given if great debility exists. In chronic cases the tonics before mentioned with the addition of the hypophosphites should be resorted to, and change of climate is very likely to be of service.
From its occurrence nearly always in females and from a supposition of its originating in some affection of the womb, this name has been given to a variable disorder, of which the main characteristic is morbid excitability of the whole nervous system.
|
|
|
|
|
|
|
Symptoms 1.—A "fit of hysterics" is a paroxysm whose nature may vary from mere uncontrollable laughter or crying to a severe epiliptiform convulsion. This last, however, differs from epilepsy in that being less complete loss of consciousness and in its curability.
2. Simulation of other diseases, indeed the assumption of severe functional disorders of different organs, is a common trait of hysteria. There may be hysterical amaurosis; hysterical insanity is not uncommon; nor is hysterical paralysis or coma rare. Retention of urine, cough, aphonia, and so forth, are often thus produced.
Catalepsy.—Catalepsy or trance is a condition allied to hysteria in some respects, in which the whole frame lies prostrate and helpless, or that a limb, if lifted up, falls back as if it were relaxed and dead while yet the consciousness of the person affected may be retained without the sensitiveness to physical pain. This curious state of existence is not well understood, and in our present ignorance of its nature the chief importance lies in its being distinguished from death early enough to prevent that most horrible of all human misfortunes, being buried alive.
Hypochondriasis.—This is a very obstinate affection, often hereditary, and occurring more frequently in men than in women. During the attack there is apparently great depression of mind without mental disease. The patient imagines he is afflicted with maladies of the most varied kinds; is tormented with ideas of impending miseries and dangers; thinks he suffers from swellings or contortions of the body, which may be purely creations of fancy. This disorder in the male corresponds very nearly to hysteria in the female, and like it can only be cured by attention to the general health. Tonics, exercise and cheerful occupation are the best remedies.
Treatment of Hysteria.—Much skill and care will often be required in the management of hysteria, as each one has peculiarities of its own. Generally a tonic regimen is demanded. Iron and cod-liver oil are most often the appropriate remedies. Bromide of potassium is sometimes quite useful. For a paroxysm of "hysterics" asafetida is universally safe and reliable in pills of three grains each. Sinapisms and pediluvia are also proper. Menstruation is often irregular in hysterical women; it should be regulated as far as possible. Exercise in the open air, as a rule, is very important for such persons. Mental and emotional excitement should be avoided; but tranquil, even engrossing, occupations will be beneficial. For hysterical paralysis electricity is promptly useful. Cold bathing, especially the shower-baths or sea-bathing, when followed by reaction, will do good.
|
|
|
|
|
|
|
Meaning.—Pain, without inflammation or other disorder, except that of the nerve or nerve-centre involved; literally nerve pain. This may affect any of the sensitive nerves. It is also sometimes referred to parts which have, in health, no sensibility; as the heart, stomach, and so forth. Different names are given according to its site. Thus, tic douleureux is facial neuralgia; hemicrania, that affecting one side of the head; sciatica, that of the hip; gastrodynia, neuralgic pain in the stomach; pleurodynia, in the side. Angina pectoris is, chiefly, a neuralgic affection of the heart.
Symptoms.—The pain is generally acute shooting or darting, with tenderness of the part upon pressure. There is, however, no heat or swelling, or throbbing of the blood-vessels in pure neuralgia. Complicated cases occur in which inflammation and neuralgia exist together, and inflammation of the fibrous neurilemma may be the immediate cause of the neuralgic pain.
Causes.—Neuralgia is always dependent upon debility arising from one cause or another, as, for instance, anemia, mental anxiety, gout, rheumatism, syphilis and dyspepsia. In fact, a great German authority upon nervous diseases declares, with as much truth as poetry, that "neuralgia is the prayer of the nerves for iron in the blood."
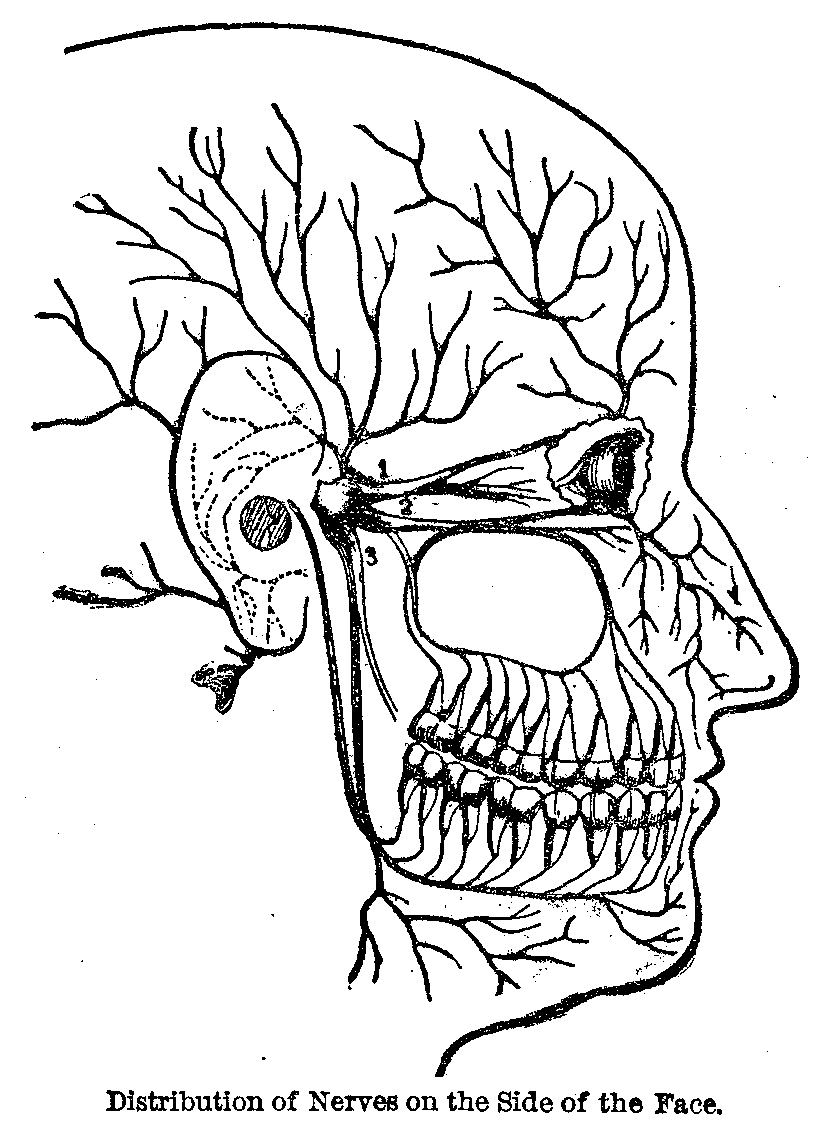
Next to the sciatic nerve no other is so often the seat of neuralgic pain as the trifacial, and this is, perhaps, partly owing to the fact that the superficial branches are spread out over a large surface upon the side of the face and more exposed to cold and changes of the weather than any other part of the body where the epidermis is equally delicate. Terminal branches of the trifacial come out through the bones of the head at points over the eye, beneath the eye and at the side of the chin—as shown in the marginal illustration. These, then are the tender points, where all the branches of this nerve are involved in the neuralgia, and it is from these points that the darting bony pains seem to radiate.
|
|
|
|
|
|
|
Hemicrania or Migraine.—This is a combination of neuralgic symptoms with ordinary headache occurring in paroxysms, and usually limited to one side of the head or brow. It is apt to commence in childhood and go on to advanced age, occurring in both sexes, but more often in women than in men. In women the attacks are especially apt to appear just before the menstrual period or during its course.
Causes.—The headache is probably due to excitement of the sensitive filaments of the trifacial nerve—distributed to the dura mater—and also to the sympathetic fibres accompanying the blood-vessels, which connect the nervous supply of the brain with that of the stomach so intimately.
Symptoms.—As generally manifested it increases rapidly soon after waking in the morning with chilliness, loss of appetite, sliminess of the mouth, sickness of the stomach, vomiting of a little greenish fluid, and at last the headache becomes so intense as to be almost unbearable.
Sciatica.—This is often associated with both rheumatism and gout, but is also frequently brought on by catching cold. Occasionally it is due to accumulations in the bowels, or to diseases of the bones through which the nerve makes its exit. The painful points are usually found back of the trochanter or most projecting point of the thigh bone, at certain spots in the thigh about the knee and ankle joints.
Intercostal Neuralgia.—This, like intercostal rheumatism, resembles the pain of pleurisy and of pneumonia, and has often given rise to unfounded anxiety as to the existence of these more dangerous diseases. It may be at once distinguished by careful examination of the lungs.
Neuralgias of the arm, neck, shoulder, and so forth, are all unhappily common and sometimes very intractable.
Pathology.—At least three sources of pain are possible. 1st. Local disease affecting a nerve. 2d. A morbid state of a sensorial nerve centre, 3d. A morbid condition of the blood. Neuralgia always fixed or returning in the same spot, is likely, although not certain, to depend upon a fault in the nerve itself; as neuroma (tumor of a nerve). Radiating pain must at least involve part of a nerve centre. Flying pains, never long seated in one part of the body, are due to a defect or morbid poison (as that of gout or malaria) in the blood.
Treatment of Neuralgia 1.—This must, of course, depend upon the cause or nature of the case. Tic douleureux often depends upon decay of the teeth; if so, they must be attended to. Other purely local neuralgias require local treatment. Laudanum or paregoric, applied by saturating a cloth and laying it upon the part covered by oiled silk to prevent evaporation, is an efficient local anodyne. So is chloroform, similarly applied; it is very pungent, burning like mustard. Sinapisms will sometimes relieve promptly.
|
|
|
|
|
|
|
2. Mere warmth, as of flannel steeped in hot water, will do in some instances. Rubbing for a few moments with saturated tincture of aconite root until the skin tingles, or the application of ointment of veratria, twenty grains to the ounce of vaseline, may be used in severe cases. In the most obstinate ones a blister may be applied, dressed, after removal of the cuticle, with two grains of the acetate of morphia, diluted with ten grains of gum arabic. Carbolic acid is a powerful local anesthetic, though (unless diluted with oil or glycerine) very irritating to the skin; or, most prompt usually of all, solution of morphia may be hypodermically injected.
3. Of anodynes internally used, belladonna has, for neuralgia, the greatest reputation. It will not quell suffering so directly as opium or morphia, but it will more entirely do away with the neuralgic state. For this, however, iron, especially in combination with quinine or strychnia, is the most effective medicine. Cases of neuralgia which will not be benefited by iron are decidedly exceptional.
4. In some instances application of the galvanic current will remove the pain of neuralgia as if by magic, and when relief can thus be secured it is far preferable, as the distressing sickness, headache and constipation, which so often result from opium and other narcotics, may thus be avoided.
Auxiliary Treatment.—The hygienic treatment is almost equally important with the medicinal, and a thorough examination of the habits of life pursued by the patient will almost always lead to the discovery of some violation of sanitary law, which must be corrected before a hoped-for cure can be realized.
PRESCRIPTION 1.
Rx.---Menthol .................................. 20 grains
Muriate of cocaine........................ 10 "
Chloral .................................. 5 "
Vaseline ................................. 3 drachms
Apply the ointment to face where pain is seated.
PRESCRIPTION 2.
Rx.---Citrate of caffeine....................... 15 grains
Phenacetine .............................. 1/2 drachm
Make ten capsules. Take one every 2 or 3 hours.
|
|
|
|
|
|
|
PRESCRIPTION 3.
Rx.---Carbonate of iron........................ 2 drachms
Sulphate of quinine...................... 5 grains
Extract of opium......................... 3/4 grain.
Make 20 pills. Take 5 or 6 during the day.
Causes.—May arise under two different conditions or circumstances. Where stimulants are suddenly withdrawn from one accustomed to them; and, while their use in excess is continued.
Symptoms.—Sleeplessness, debility, tremors, horror, hallucinations, often with loss of digestive power. The insomnia is a cardinal symptom; if the patient sleeps a whole night he recovers. Debility varies in degree in different cases; in a first attack it is not always great, tremor is nearly always present. The illusions of the patient are wonderfully real, and usually dreadful. He is pursued by demons or beset by moral enemies; he cannot bear to be alone, especially in the dark. Sometimes, however, the visions are indifferent, or even amusing.
Treatment.—If the patient be not much prostrated, give only ale or porter, a bottle or two in the day, with hop tea ad libitum and a grain of opium every three or four hours. Very weak patients, accustomed to spirits, might have a tablespoonful of whiskey or brandy every two, three or four hours, according to their condition. Hydrate of chloral sometimes answers as well as, or better than, opium. Digitalis has been used in some cases with great boldness, in doses of half an ounce of the tincture, repeated when necessary in four hours; as soon as the remedy produces its full effect sleep for five or six hours commonly follows. Sleep is the guide to the repetition of the dose.
Diet.—Beef tea and mutton broth, and so forth, seasoned with red pepper, are preferred as diet. In an obstinate case sleep may follow the raising of a blister upon the back of the neck. Substituting valerian for opium, or combining the fluid extract or tincture of valerian with morphia solution answers well in some cases. Injection of laudanum into the rectum is occasionally resorted to. Success in treatment has been obtained from the use of chloroform in doses of one or two drachms. The corrugated stomach of a spirit drinker will probably bear the pungency of chloroform better than anetheis. The large majority of first attacks of mania-a-potu are curable. Third and fourth attacks are often fatal, or are followed by permanent insanity.
|
|
|
|
|
|
|
PRESCRIPTION 1.
Rx.---Indian hemp .............................. 10 grains
Divide into 12 pills. Take one every 2 or 3 hours
until drowsy.
PRESCRIPTION 2.
Rx.---Hyoscyamus .............................. 1 grain
Alcohol ................................. 1 drachm
Water ................................... 1 "
Inject 5 to 10 minims with hypodermic syringe.
Causes.—1. This consists chiefly in a particular organization of the brain and nervous system, rendering those individuals so constituted liable to become insane when exposed to the influence of certain agencies, which in other persons either give rise to a different train of morbid phenomena, or are, perhaps, devoid of any injurious effects.
2. Among the agents which give rise to madness there is none more influential than intemperance, or the frequent use of ardent spirits. That the predisposition to madness, when it has once arisen, is frequently transmitted, is a fact too well established to admit of doubt.
3. The exciting causes of insanity may be divided into moral or psychical and physical. The principal psychical are grief, fright, anxiety, care, or an excited state of any passion; the emotions aroused by disappointment, excessive or prolonged employment of the intellectual faculties, and so forth. Anything which will produce a hyperemia of a portion or the whole of the brain by which the nutrition and consequently the normal function is interfered with.
4. The principal physical causes are drunkenness and the use of narcotic or poisonous drugs, want of food, want of sleep and over-exertion; other nervous diseases such as epilepsy, chorea and hysteria; severe injuries to the head, particularly from blows, causing fracture of the skull or concussion of the brain, sunstroke and tumors in the brain. Acute febrile diseases as typhoid, typhus and malarial fevers, and it may occur during the course of pneumonia in the form of acute mania. The poison of Asiatic cholera may so interfere with the nutrition of the brain as to produce not only transient delirium but mania, which may continue several days or weeks. Acute rheumatism is sometimes a cause, chronic constitutional diseases are frequent causes, and among the most formidable of these is constitutional syphilis. Diseases of the genital organs sometimes exert an important influence in producing insanity.
|
|
|
|
|
|
|
Symptoms 1.—The earliest symptoms of coming insanity are depressed manner, unusual excitement, anger and rashness.
2. An important symptom in all forms of insanity is impairment of the faculty of attention. The inconsistency of the beliefs of the insane is one of the earliest noticeable symptoms, and they are classed as "delusions" and "hallucinations." A delusion is a false belief in regard to some fact which generally concerns the patient, and which is so strongly rooted that all attempts to reason him out of it are futile. A hallucination is a false perception of one of the senses; the patient may fancy that he sees a spirit or a person who does not exist.
Melancholia.—This may be acute or chronic and is marked by extreme depression of both mind and body. The first stages of melancholia are generally preceded by a condition called hypochondriasis, which may be considered as the mildest form of insanity. There is a feeling of bodily illness at this time more than at any other, or in any other form of insanity.
Treatment 1.—The treatment of a case of chronic or subacute melancholia will vary with its history and symptoms. An asylum is not indispensable if the patient's means are sufficient to provide him with proper care. He may be benefited by travel and change of scene; but when his condition will not admit of this a proper place, either a private house or an asylum, should be selected, and an attempt made by therapeutical and hygienic measures to restore the cerebral defect by sleep and nourishment of the body.
2. There are three conditions which require constant attention: want of sleep, rejection of food and constipation. To remedy the first chloral is most beneficial. The practical aim is to produce sleep, regularity of the evacuations by laxative medicines and to sustain the strength with nourishing food and wine.
Mania.—There are two varieties, the acute and chronic. In the acute form the excitement is extreme, and follows closely upon the delusion or derangement of ideas. In the chronic form the delusion or derangement is confirmed but less obtrusive, while the excitement is subdued or comes on at long intervals. Mania has generally a sort of stage of incubation, during which sleeplessness is one of the most important and earliest symptoms. In another class of patients the primary symptoms are those of gloom and despondency, out of which the maniacal excitement appears to develop. In both varieties there is generally a marked departure from the individual's usual state of physical health. The different forms of mania in which the disposition to commit murder, suicide or arson, or to steal, is quite uncontrollable, are well known. When a single tendency of this kind is very prominent the case is usually denominated one of monomania.
|
|
|
|
|
|
|
Treatment.—The treatment consists in regulating the bodily functions, giving food freely, combined with plenty of drink, also wine, and in the judicious use of chloral. Rest is of the highest importance, and baths of warm water are of great benefit, the head to be kept cool during the operation. Purgatives at the outset of the attack may be of use, as aiding to arrest it.
PRESCRIPTION.
Rx.---Fluid extract of conium................. 1-1/2 drachms
Fluid extract of hyoscyamus............. 1-1/2 "
Hydrate of chloral...................... 2-1/2 "
Syrup of orange peel.................... 1-1/2 ounces
Take a teaspoonful every 2 or 3 hours, as occasion
requires.
Dementia.—Dementia is literally a want of mind, and the word indicates a condition in which there is feebleness of intellectual grasp, or attention, imbecility of word and act and general deficiency of mental power. It is one of the common terminations of both mania and melancholia, and if long continued, its outward signs are a vacant and puzzled look, a lack-lustre eye, a weak smile and a meaningless laugh. This kind of insanity is almost a natural termination of extreme old age and is then called senile dementia. Not infrequently the subjects of it become paralytic.
Imbecility.—Imbecility is a condition in which the mind is from birth unfitted for the active and thoughtful duties of life, and in which the person affected is said to be half-witted, or wanting in general intellectual capacity. This condition of deficient mental development may be associated with moderately good physical health in early life, but there seems to be usually some taint in the system, so that the family of imbeciles is, as a rule, short-lived, the members dying early of consumption, diabetes or some degeneration of the brain and spinal cord.
Idiocy.—Idiocy is a still lower grade of mental weakness, in which the intellectual faculties are below the standard necessary for reasonable life. In the true idiot the head is of a reduced size and the appetites and propensities are very little, or not at all, controlled by reason. Many idiots are deaf and dumb, but most of them retain their sight. The sad condition of these poor creatures may be often ameliorated by systematic training, but complete cure after puberty is hopeless.
|
|
|
|
|
|
|
Treatment of Insanity.—The treatment of insanity is generally best carried out in asylums for the purpose. To quiet a patient temporarily, or on his way to a suitable institution, bromide of potassium in quantities of thirty grains, or chloral in fifteen-grain doses every two or three hours, morphia by hypodermic injection, or otherwise, and even chloroform by inhalation may be necessary,
This page is maintained by
Charles Keith.
Contact:
Send me a message
Last Modified: Monday, 13-May-2013 15:31:46 EDT