|
|
|
|
|
|
|
New Medical Views.—Affections of this class were, until recently, supposed to present symptoms of very much the same general character, and therefore to constitute a class of maladies which possessed considerable unity in their intrinsic nature. They are now, however, found to consist of a variety of distinct affections producing very different and sometimes opposite symptoms. Thus hypertrophy produces increased and dilatation diminished force of the circulation. In order, therefore, to appreciate the value and familiarize ourselves with the nature of each class of symptoms, it is necessary to study the several affections in an isolated form. We are thus enabled, on meeting with a compound case—one consisting of a complication of several of the simple affections— to analyze or unravel the symptoms, ascertain the relative importance of each class, and in this manner establish rational and secure principles of treatment. In conformity with this view, the various articles on the diseases of the circulatory and absorbent systems, instead of being assembled under the present head, are, for facility of reference, diffused alphabetically throughout the work.
Hearing the Heart-Beats.—If we apply the ear, with or without the stethoscope, to the cardiac region of a person in health, we perceive most distinctly a series of sounds of a very marked and peculiar kind, subdivided into uniform parts by a brief interval of silence after every second sound. Two sounds follow each other instantly, or within so short a space that the ear separates them rather by difference in their quality than from the intervention of any notable cessation of sound; then ensues a brief but well-marked pause, which is again succeeded by the first of the time sounds. This series of sounds may be perfectly well represented, as to rhythm, by musical notation. The relative duration of the sounds and pause is represented by Lawrence to be nearly as follows: the whole being divided into four parts, two of these are occupied by the first sound, and one by the second sound and the pause respectively.
|
|
|
|
|
|
|
Difference in the Sounds.—The two sounds differ in kind as well as in duration. The first is nearly double the length of the second, of a graver and more subdued tone, rather louder at its commencement than at its termination, as if it was about to die away, when suddenly interrupted by the second. The second is brief, smart and clear, like a gentle tap with the pulp of the finger on a solid table, or like the sharp sound produced by the pulling back of a valve, the cracking of a whip, or the lapping of a dog. Exactly synchronous with the first sound, there is perceptible, in most cases, a well-marked impulse or shock communicated evidently by a body in motion within, in the walls of the chest. Every one acquainted with anatomy and physiology will at once conclude that the sounds and impulse just described are produced by the motions of the heart; and this conclusion will be justified and confirmed by an examination of the pulse in the extremities. It will be found, in all healthy subjects, that there is an invariable connection between the sounds and the pulse; every stroke of the latter corresponding very accurately with every repetition of the twin sounds; as, under every variation of circumstances as to loudness, frequency, and so forth, the same exact relation is perceived, it cannot be doubted that there exists an essential physical connection between the causes of the sounds and the pulse.
Rhythm of the Heart.—The first motion of the heart which interrupts the interval of repose is the auricular systole. It is a very slight and brief contractile movement, more considerable in the auricular appendix than elsewhere, and propagated with a rapid vermicular motion toward the ventricle, in the systole of which it terminates rather by continuity of action than by the succession of a new movement. The ventricular systole commences suddenly and is accompanied with a considerable diminution of the volume of the organ. Synchronous with the systole are the first sounds—the impulse of the apex against the ribs and the pulse in vessels near the heart; in the radials the pulse follows at a barely appreciable interval.
The Diastole Motion.—The systole of the ventricles is followed by their diastole, during which they return, by an instantaneous expansive movement, sensible to the touch and sight, to the same state (with respect to size, shape, position, and so forth), as during the previous interval of repose. This movement, or diastole, is accompanied by the second sound, by an influx of blood from the auricle, by a retractile motion of this cavity most observable at its sinus, and by a retrocession of the apex of the heart from the walls of the chest. Next succeeds the interval of repose, during which the ventricles remain at rest, in a state of fullness, though not of distension, through the whole period intervening between the second and the first sounds; but the auricle remains at rest during the first portion only of the period, the remainder being occupied by its next contraction, with which recommences the series of actions described.
|
|
|
|
|
|
|
1. The ventricular systole occupies half the time of a whole beat.
2. The ventricular diastole occupies one-fourth or one-third.
3. The interval of ventricular repose occupies one-fourth, or rather less, during the latter half of which the auricular systole takes place.
Causes of the Motions.—The auricles, which are always in a state of fullness, arrive, during the first half of the period of ventricular repose, at the state of distension, by which they are stimulated to contract. The object of the contraction at this movement is to propel a small additional quantity of blood into the ventricles for the purpose of bringing them from the state of fullness to that of distension; an object which could not be accomplished without a contraction, as the blood could not otherwise force its way into the ventricles against the resistance offered by their elasticity. The cavities, then, being brought to the state of distension, are by this stimulated to contract; they expel a greater or less proportion of their contents; in small animals—frogs, for instance—they expel the whole; which is proved by the ventricle being full. In larger animals they no not appear to expel the whole, but the fact does not admit of demonstration. During the act of expulsion, the apex is tilted up, in consequence of the retraction of the ventricles toward the base and upon the auricles, which, in a state of extreme distension, are placed like a fulcrum beneath them.
Causes of Diastole Motion.—The diastole appears to be occasioned by several concurrent causes, viz.:
1. That power of the muscle by which it reverts from the state of contraction to that of relaxation, and in virtue of which it exercises a degree of motion. It may be called elasticity.
2. The distension of the auricles, which is greater at this moment than at any other, as they have been filling during a longer period; namely—that of the ventricular contraction, or half a whole beat.
3. The weight of the ventricles collapsing on the distended auricles underneath them.
(Continued on page pg0420)
|
|
|
|
|
|
|
FIGURE NO. 1.
1. External or muscular tunic of the upper right cavity of the
heart (right auricle).
2. External or muscular tunic of the left upper cavity (left
auricle).
3. External or muscular tunic of the right lower cavity (right
ventricle).
4. External or muscular tunic of the left lower cavity (left
ventricle).
5. Upper cava vein, or conduit which carries the blood from the
upper part of the body to the heart.
6. Under cava vein, or conduit from the lower part of the body.
7. Pulmonary artery.
8. Aorta.
9,10. Coronary arteries.
11. Division seat between the right and left ventricles.
12. Series of vessels for feeding the external part of the
heart.
13. Position of the valves of the heart.
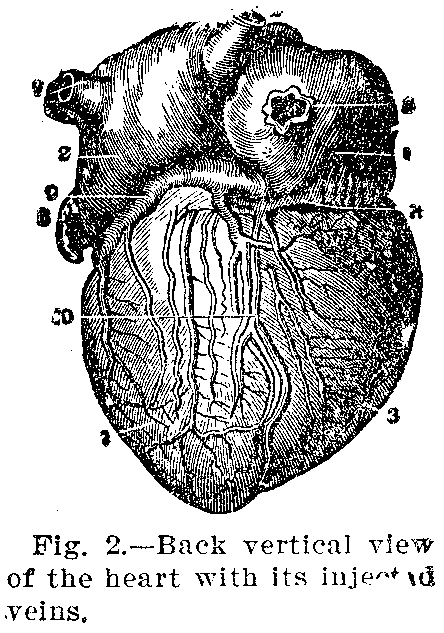
FIGURE NO. 2.
1. Back part of the right auricle.
2. Back part of the left auricle.
3. Back part of the right ventricle.
4. Back part of the left ventricle.
5. Opening of the upper cava vein.
6. Aorta.
7. Pulmonary artery.
8. Lower cava vein.
9. Vessel for feeding the walls of the heart.
10. The same.
11. Position of the valves of he heart.
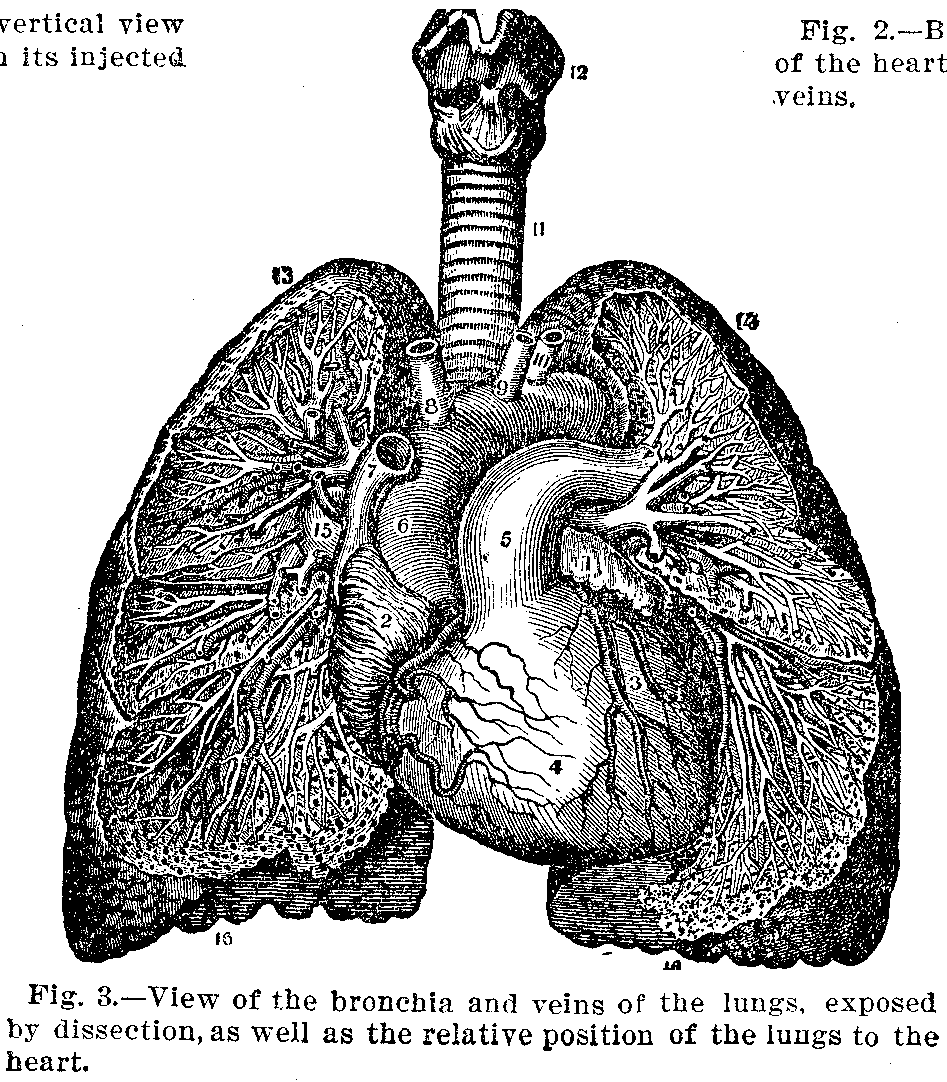
FIGURE NO. 3.
1, 2, 3, 4, 5, 6, 7, 8, 9, 10. Parts and vessels of the heart as
demonstrated in Figures Nos. 1 and 2.
11. Windpipe (larynx).
12. Cartilages and seat of the vocal cords.
13,14. The lungs in their upper part, called the apex.
15. Branches, in the lungs, of the greater blood-vessels.
16,16. Base of the lungs, showing the exterior surface.
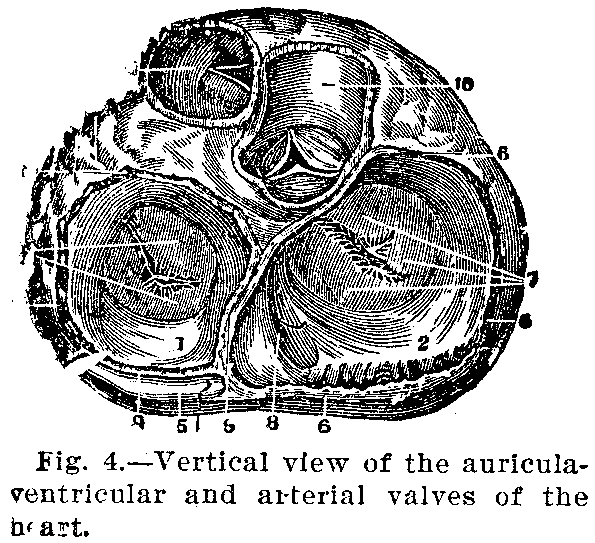
FIGURE NO. 4.
1. Cavity of the auricle.
2. Cavity of the ventricle.
3,3,3,3. Muscular tunics.
4. Tricuspidal valve.
5. Pulmonary artery.
6,6,6. Inner tunic of the heart.
7. Mitral valves.
8. Auricula-ventricular opening.
9. Dividing wall.
10. Aorta.
11. Cava vein.
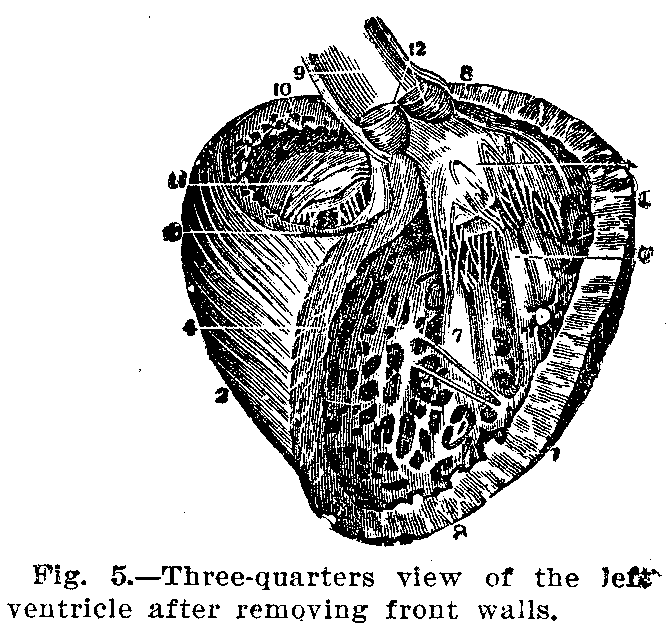
FIGURE NO. 5.
1,2,3. Pericardium.
4. Muscles of the wall of the heart.
5. Plaits of the lining of the heart.
6. Tendon cords.
7. Fleshy columns.
8. Seat of the valves.
9. Opening facing the auricle.
10. Walls surrounding the mitral valve.
11. Mitral valve.
12. Semilunar valves.
|
|
|
|
|
|
|

For an explanation of the illustrations see text on opposite page.
|
|
|
|
|
|
|
4. The width of the auricula-ventricular orifice, which allows the blood to shoot in instantaneously and with great facility.
It is obvious that, as so many powerful causes conspire to promote the influx of the blood, an auricular contraction for this purpose would be superfluous. The escape of blood from the auricles during the diastole causes the slight retraction observable in them at the same moment. The expelled blood being instantly replaced from the vena cava, distension of the auricles recommences, and the same series of actions is renewed.
Causes of the Sounds.—The ventricular systole is the cause of the first sound, by the impulse which it communicates to the blood within it, thereby exciting sonorous vibrations of the fluid. If the sound of the muscular contraction contributes at all to the first sound it can only be in a very slight degree. The ventricular diastole is the cause of the second sound, by the reaction of the walls on the blood, and the consequent production of sonorous vibrations, when its cause is abruptly arrested by the completion of the diastole. Hence this sound is loud, brief and clear. The auricles are not concerned in the production of the two sounds, as they take place when these cavities are motionless; nor do they appear to be productive of any sound, as no third sound is audible.
Auscultation or Sounding.—We now proceed to examine more minutely the phenomena produced by the actions of the heart, in health and disease, with the view to deduce therefrom such diagnostic signs as they are capable of affording. It is hardly necessary to premise that the auscultatory diagnostics of cardiac diseases are founded precisely on the same principles as those which apply to diseases of the lungs.
Physical Signs.—Disturbance of the functions of the heart must necessarily produce decided effects throughout the whole circulatory apparatus. Appreciable modifications of the arterial pulse of the state of the veins and capillaries show that the circulation is embarrassed. The pulse irregular, unequal and intermittent, as are the pulsations of the heart very small; but when there is considerable hypertrophy of the left ventricle, the pulse is also hard and vibrating, presenting sometimes a peculiar fremitus, which is most distinct in the carotid, subclavian and radial arteries. In some cases the arterial pulsations succeed one another, stroke by stroke, and this reduplication of the pulse is coincident with a regurgitant murmur heard on auscultating the heart. The insufficiency of the aortic valves is characterized by a bellows-murmur at the base, accompanying the second sound of the heart, and by a bounding pulse with flexuosity of the radial artery.
|
|
|
|
|
|
|
Symptoms.—When disease of the heart has reached a pretty advanced stage, the existing impediment to the venous circulation is indicated by swelling of the veins near the heart; those, for example, of the neck and face; and this turgescence is particularly obvious in the external jugular veins, where it is sometimes accompanied by undulatory pulsations, analogous to and synchronous with the arterial pulse. This is the venous pulse indicative of hypertrophy of the right ventricle.
Further Symptoms.—In addition to the embarrassment of the venous, there is embarrassment of the capillary circulation, which declares itself by a livid tint of the skin, swelling of the face, puffiness of the eyelids, a bluish color of the lips, and more or less injection of the skin of the extremities.
Palpitation.—As palpitation is under all circumstances dependent on over-excitement of the nerves of the heart, the phenomenon is always essentially the same. The varieties which it presents arise merely from differences in the causes and from the different routes which these causes pursue in order to arrive at and convey their stimulus to the heart.
Blue Skin.—Cyanosis is a morbid appearance which consists in the skin assuming a blue, purple or violet color, especially in those parts where the cutaneous capillary vessels are superficial, as on the cheeks and lips. It is generally accompanied by difficult respiration, palpitation of the heart with diminution of the natural temperature, an irregular or intermitting pulse, and is often attended with dropsical symptoms, the face especially, in addition to the purple color, being bloated and edematous; all these symptoms are much aggravated by any exertion.
Intensity of the Disease.—Its intensity varies considerably in different cases, being sometimes excruciating and sometimes slight or even wanting. There is also more or less tenderness on pressure over the region of the heart, and its action is notably increased. With these local symptoms are associated those pertaining to the system at large which accompany symptomatic fever. As the affection is almost always developed in connection with other diseases, the symptoms of the latter are of course combined with those of the former.
Diagnosis.—The diagnosis or recognition of pericarditis has been rendered prompt and positive by means of auscultation and percussion. Soon after the attack the exudation of fibrine occasions a friction sound with the heart's movements, and this is proof of the existence of the disease. Afterward, when considerable liquid has been effused into the sac, the friction sound may cease, but it is practicable to determine the presence and the quantity of liquid within the sac by physical signs, which are obtained only by auscultation and percussion. The danger in cases of pericarditis depends, other things being equal, on the intensity of the inflammation, the quantity of exuded fibrine and the amount of effused fluid. Aside from these conditions, much depends on the diseases with which it is associated.
|
|
|
|
|
|
|
Symptoms.—When developed in connection with rheumatism, it ends in recovery in the majority of cases; but occurring in connection with diseases of the kidneys, with pleurisy or pneumonia, and in cases of pyemia, it ends in death much oftener than in recovery. When death is not sudden, the disease destroys life by slow asthenia or exhaustion.
As a rule from the outset we have acute inflammatory fever, a pungent, burning, lancinating pain in the region of the heart, shooting to the left scapula, shoulder, and upper arm, but rarely descending below the elbow, or even quite to it. The pain is increased by full inspiration, by stretching the left side, and especially by pressure between the precardial ribs, and by forcing the epigastrium upward underneath the left hypochondrium. When the inflammation is only subacute the pain is more or less dull, and does not lancinate. There is inability of lying on the left side, and sometimes in any position but one, which is most commonly on the back, dry cough, hurried respiration, palpitation of the heart, the impulse of which is sometimes violent, bounding and regular, though its beats may at the same time be unequal in strength, at other times it is feeble, fluttering and irregular, pulse always frequent, and generally, at the outset, full, hard, jerking, and often with a thrill.
Causes.—The most frequent causes are blows or excessive pressure in the pericardial region, inflammation propagated from the lungs or pleura, and far above all, rheumatism. From this cause children and young persons suffer much oftener than others. The remaining causes are those of inflammation in general, viz., cold, febrile excitement, and so forth.
Treatment.—As regards treatment, acute pericarditis claims in general the measures indicated in other inflammatory affections. The antiphlogistic treatment, in as energetic a form as circumstances will allow, should be employed with the utmost promptitude. The loss of a few hours at first may be irretrievable, and hence hesitation and indecision may seal the fate of the patient. These measures, however, are in many cases to be modified by the circumstances pertaining to the diseases with which this is associated.
|
|
|
|
|
|
|
Strength of the Remedies.—The strength of the remedies employed must in each case be apportioned to the vigor of the patient's constitution; but the object is the same in all, expeditiously to prostrate the action of the heart, and for a time to keep it prostrate by preventing the reestablishment of reaction. If this object can be accomplished for the first twenty, thirty or forty hours, the disease frequently does not rally, but remains perfectly under the control of remedies.
Additional Treatment.—In addition to the above measures diluent cooling drinks—as four scruples of bitartrate, or two of nitrate of potassa in a quart of water, and flavored at pleasure—should be allowed in unlimited quantity, in order by diluting the blood to render it less stimulant to the heart. Nauseating doses of tartrate of antimony, as one-sixth to one-eighth of a grain every two hours, may be employed with advantage. Colchicum often proves useful, especially so when the disease is of rheumatic origin. Calomel, trusted still by some and abused by others, may be confined to open sthenic cases in previously good constitutions. Where the rheumatic diathesis is marked alkalies will be indicated. Carbonate or bicarbonate of potassium, or bicarbonate of sodium, may be given in scruple or half scruple doses, with as much of rochelle salts, three or four times a day.
Continued Treatment.—Should pain continue in the advanced stages of the disease, blisters may be resorted to, and repeated in quick succession, with great advantage. For the stage of effusion we have occasionally found a third or a fourth necessary, combined with the use of diuretics, as squills, juniper, sps. arth. nit., and so forth, varied and continued until absorption occurs. Tonics will often promote the same end.
Convalescence.—An individual who has recently been affected with pericarditis is peculiarly liable to a recurrence of it, especially if it has resulted from rheumatism, and if the reparation has been incomplete. In this case, should rheumatism return, it rarely fails to be accompanied with a renovation of the pericarditic symptoms.
Diet.—A very spare unstimulating diet and extreme tranquillity must be imperatively enjoined until the action of the heart has become perfectly and permanently natural. This should consist wholly of the weakest slops, as barley, water gruel, weak tea, arrow root, and so forth.
Chronic Peculiarities.—Chronic pericarditis may be a sequel of the acute affection, or the inflammation may be subacute from the first. In some cases the inflammation continues with an abundant exudation of lymph, agglutinating the inner surfaces of the sac, and proving fatal by slow exhaustion. In other cases a large accumulation of liquid takes place, amounting to several pounds in weight, and to the exhaustion incident to the persistence of the inflammation is added the compression of the heart thus occasioned. In both varieties the disease, as a rule, proves fatal sooner or later.
|
|
|
|
|
|
|
Treatment of Chronic Pericarditis.—A rapidly depressing case of pericarditis, with cold, blue skin and feeble, irregular pulse, will require, instead of the above, a supporting or stimulating treatment from the first; with dry cups and blisters instead of local or general bleeding; and quinine, ammonia and whiskey, instead of sudorifics or laxatives.

Signs of the Disease.—Inflammation of the internal membrane of the heart. In this affection the inflamed membrane is in contact with the blood contained within the cavities of the heart; hence, although fibrinous exudation takes place as in pericarditis, the exuded lymph is in a great measure washed away from the membrane and carried into the circulation. A portion, however, adheres to the membrane roughening the surface in contact with the blood, and giving rise to an abnormal sound (an endocardial or bellows murmur), which is an important physical sign of the disease. Moreover, upon the little masses of lymph which adhere to the membrane, coagulated fibrine from the blood contained in the cavities of the heart is apt to be deposited, and in this way are produced the so-called vegetations or warty growths, which being sometimes detached and carried into the arteries with the current of the blood, are arrested in vessels too small to allow of their further progress, become fixed and occasion an obstruction which may lead to hemorrhage (hemorrhagic infarctions), and to the impairment of nutrition within a circumscribed area beyond the point at which the obstruction is seated. These movable plugs or emboli, as they are termed, play an important part in affections proceeding from disturbance of the circulation and nutrition in different organs of the body, more especially the brain.
|
|
|
|
|
|
|
Local Effects.—The local effects of endocarditis are also of much importance as laying the foundation for progressive changes, especially in the valves of the heart, constituting what are called valvular lesions. The inflammation in endocarditis is generally limited to the left side of the heart; that is, to the endocardial membrane lining the left ventricle and the left auricle.
Causes.—Like pericarditis, this is very rarely a primary disease, and in the great majority of cases it occurs in connection with acute articular rheumatism. It is evidently due to the same internal agency which in rheumatism causes the inflammation within the joints; this agent being a morbid principle in the blood, is supposed to be lactic acid.
Diagnosis.—Its development is attended with little or no pain or other subjective symptoms referable to the heart; the diagnosis rests wholly upon physical evidence attained by auscultation. The roughening of the endocardial membrane within the left ventricle causes, as already stated, an adventitious sound or murmur, and the production of this murmur, while a patient is under observation, constitutes the proof of the presence of the affection.
Symptoms.—The symptoms produced are blueness and coldness of the skin, the result of the disease affecting the valves of the heart so as to render them more or less incompetent to perform their functions, and diminishing the size of the mitral or aortic orifice so as to produce more or less obstruction to the passage of blood. Obstruction of the flow of blood through the orifices within the heart, and regurgitation, lead to enlargement of the organ and to various morbid effects in other organs; indistinctness of the heart sound, feebleness and irregularity of the pulse, nausea and vomiting, anxiety of expression and fainting.
Treatment.—In every case the important question is, less the state of the particular valves than the amount of interference with the functional action of the heart. In young persons, remarkable recoveries sometimes take place. In other instances, adaptation of the heart itself, and of the general system by degrees, is effected, so that quite good health, and even capacity for exercise, may be attained, while the physica] signs of the local organic change remain. Sudden death is less common in heart disease than is popularly supposed.
|
|
|
|
|
|
|
The Circulation.—The circulation should be kept as tranquil as possible by a quiet life and a moderate unstimulating diet. The food, however, should be rather nutritious, comprising a little animal food or soup twice a day, in order to keep the muscular system in general, and that of the heart in particular, in tone. The same may be promoted by a clear, bracing, dry air. The general health and strength may likewise be improved by the occasional exhibition of bitters, mineral acid and chalybeates, with aromatics. The stomach, in particular, should be kept in good order, as its derangements, even a little flatulence or acidity, have a surprising effect in disturbing the action of the heart. The same may be said of the biliary secretion, when there is an unequal distribution of venous power, indicated by hysterical symptoms, and so forth, antispasmodics will be found useful.
Value of a Bath.—Attacks of dyspnoea are best relieved by immersing all the extremities in warm water, a blanket being thrown round the patient to promote perspiration, and fresh cool air being admitted to satisfy the craving for breath. While this is being done he should take an antispasmodic draught, composed of either laudanum, camphor, ammonia, and assafetida, combined according to circumstances. It may be repeated two or three times, at intervals of from half an hour to an hour, according to circumstances.
Diet.—For the avoidance of attacks the more important of the measures of management relate to a proper regulation of the habits of life as regards diet, exercise, and so forth. While excessive muscular exercise is to be avoided, such an amount as is taken, without discomfort, may be highly useful by improving the general condition of the system; while excesses in eating and drinking are hurtful, a deficient alimentation is not less so. In brief, the great end of treatment is to render the system tolerant of the lesions as much and as long as possible, and this end is promoted by such a course of management, hygienic and medicinal, as conduces to the general welfare of the economy.
Nature.—Certain forms of general anemia which are neither attributable to excessive antecedent hemorrhages, nor to profuse or long continued intestinal fluxes, and which cannot by symptoms be connected with any diathesic state or marsh miasmatic influences, forms of general anemia, in fact, which appear to supervene under the influence of non-recognizable causes, in which besides the debility and languor of the patient, are characterized by a bronzed hue of the integuments, and which is most strikingly apparent on the skin of the hands, penis, groin, scrotum and axilla.
|
|
|
|
|
|
|
It has been termed by Addison the bronzed disease.
Symptoms.—The malady begins slowly, and its existence is not at first perceived. The patient has difficulty in fixing with precision the date at which he experienced its earliest symptoms. Its first manifestations are general discomfort, an enfeebling of the physical and moral faculties, and a state of real languor. The arterial pulsations are small and feeble, the pulse full, soft and easily compressed. The appetite is capricious, the patient showing repugnance to animal food, or a diminished appetite. At first digestion proceeds in a normal manner, at a later stage this function is disturbed by intractable vomiting. This symptom is accompanied by pain, or at least by a painful sensation in the epigastric region. The patient wastes away, and yet the most minute examination fails to discover any sign of organic change sufficient to account for the great disturbance of health and extreme anemia which exist. Finally there is a state of extreme debility.
Treatment.—In the treatment, having no specific remedy, we are obliged to direct our measures against the symptoms of anemia; ferruginous medicines, preparations of cinchona, and a tonic regimen are indicated. Decided advantage has followed the use of a combination of glycerine, in two-drachm doses, with fifteen or twenty minims each of chloroform and tincture of chloride of iron.
Symptoms.—When the right half of the heart has received an embolus and the pulmonary artery is obstructed, collapse of the lungs, partial or entire, follows. Pleurisy, hemorrhage or bronchitis may also occur, or the symptoms may be great anxiety and dyspnoea, with reduction of the temperature of the body; a systolic murmur may be heard on auscultation; the rhythm of the heart becomes irregular, and pulsation of the jugular veins may be noticed. Giddiness may be present, with blueness and edema of the hands, feet, or both. Where emboli have become broken up and decomposed, septicemia results, commonly known as pyemia.
(Continued on page pg0430)
|
|
|
|
|
|
|
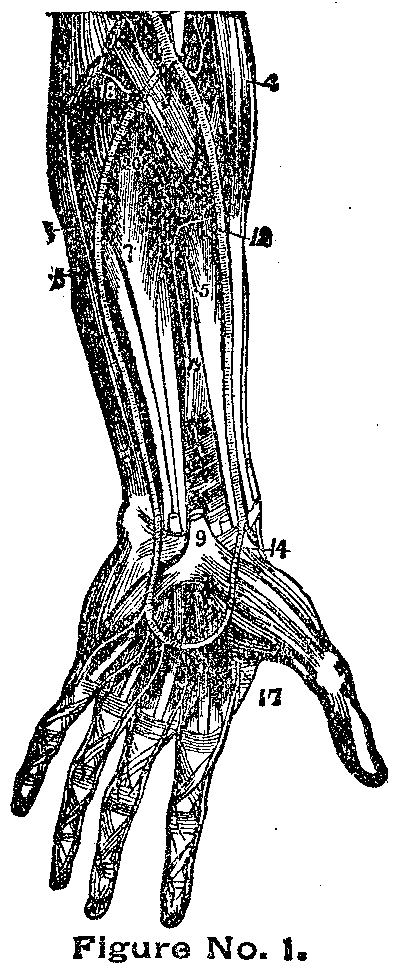
FIGURE NO. 1.---Arteries of the palm of the hand and front of
forearm
3. Deep part of the raised pronator of the radius.
4. Long supinator muscle.
5. Long flexor of the thumb.
6. Square pronator.
7. Deep flexor of the fingers.
8. Cubital flexor of the wrist.
9. Annular ligament, with the tendons that pass under the centre
of the palm of the hand; the member is on the tendon of the
long palmary muscle divided near its insertion.
10. The brachial artery.
12. Radial artery.
13. Recurring radial artery joining the end of the upper deep one.
14. Superficial veins.
15. Cubital artery.
16. Superficial palmary arch from which spring digital
branches to three and one-half fingers.
17. Magna artery of the thumb and radial artery of the index.
18. Back cubital recurring artery.
19. Front interosseous artery.
20. Back interosseous artery passing through the interosseous
membrane.
FIGURE NO. 2.
1. Primitive carotid artery dividing itself into carotid
external and carotid internal.
3. Occipital branch to the back part of the skull.
4. Upper hyoides artery.
6. Lower pharyngeal artery.
6. Masseter artery.
7. Submental artery.
8. Lower coronary artery.
9. Upper coronary artery.
10. Deep branch.
11. Back cervical artery.
12. Continuation and fold of the occipital.
13. Descending branch for muscles of the neck.
14. Posterior auricular.
15,15. Temporal artery.
16. Parietal branches.
17. Frontal branches.
19. Orbitary branches.
20. Subclavian artery.
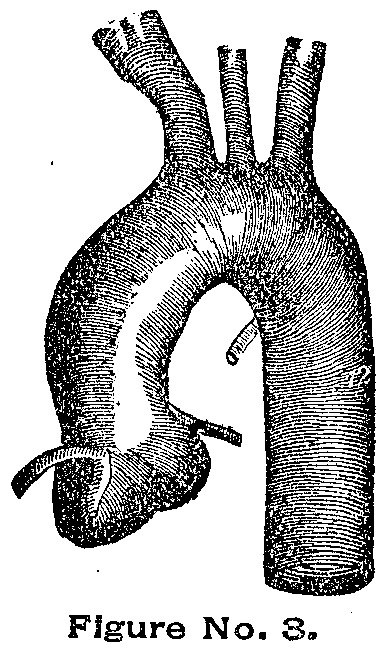
FIGURE NO. 3.
Thoracic aorta.
The three branches from left to right are the unnamed ones.
The primitive left carotid and the subclavian left one.
The small branch in the curve is the bronchial one.
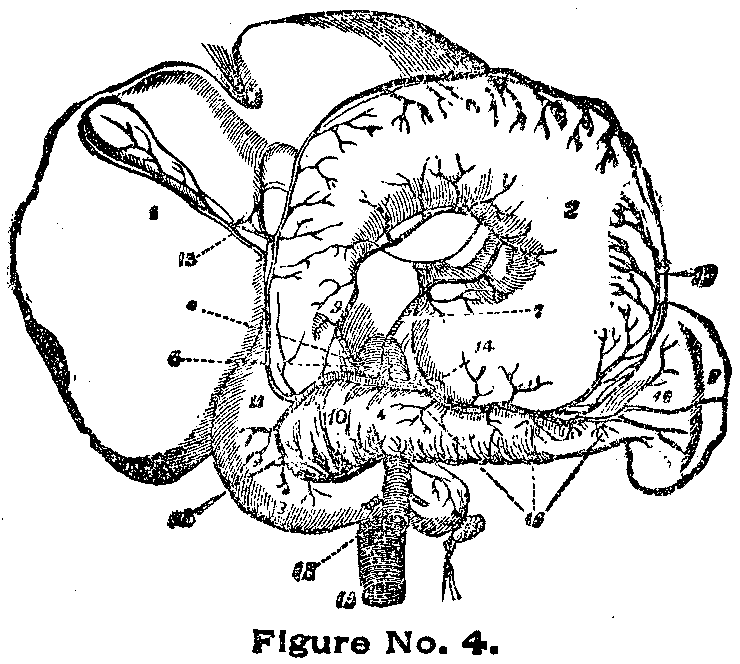
FIGURE NO. 4.
1. The liver.
2. The stomach.
3. Upper gut.
4. Pancreas.
6. Great mesenteric artery.
7. Gastric branch.
8. Spleen.
9. Pyloric branch.
10. Pancreatic branch.
11. Hepatic artery.
12. Duodinal branch.
13. Cystic artery.
14. Branches to the stomach.
15,16. Spleenic arteries.
17. Gastro-epiploic artery.
18. Descending aorta.
19. Great mesenteric artery.
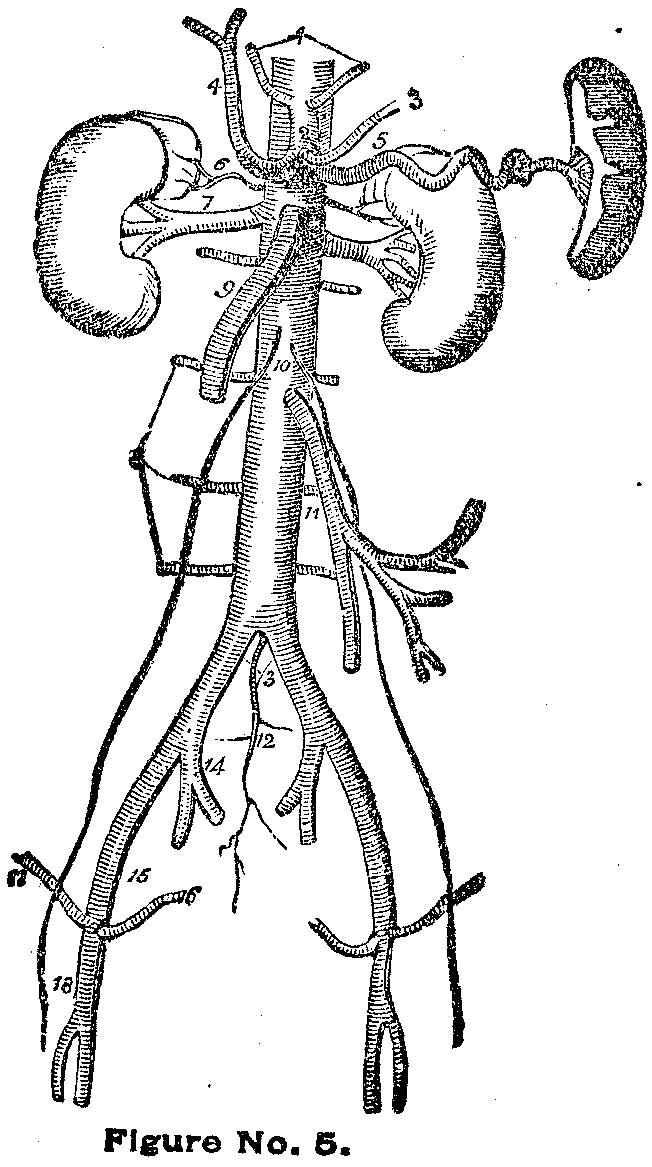
FIGURE NO. 5.
1. Cheek arteries.
2. Coeliac axis
3. Gastric artery.
4. Hepatic artery dividing itself into right and left branches.
5. Spleenic artery.
6. Supra-renal artery on right side.
7. Right renal artery, which is longer than the left.
8. Lumbar arteries.
9. Upper mesenteric artery.
10. The two spermatic arteries.
11. The lower mesenteric.
12. The middle sacras.
13. The common iliac.
14. Internal iliac of the right side.
15. External iliac.
16. Epigastric artery.
17. Circumflex iliac artery.
18. Femoral artery.
|
|
|
|
|
|
|

For an explanation of the illustrations see text on opposite page.
|
|
|
|
|
|
|
Treatment.—The objects we should have in view in the treatment of a vessel occluded by an embolus are, to favor the venous circulation through the limb by its elevation, and to establish the arterial collateral circulation by maintaining the warmth of the limb by means of cotton carefully wrapped round it over oil lint. Pain can be relieved by sedatives, while the powers of the patient are to be maintained by nutritious diet, by stimulants carefully administered and by tonics. When gangrene has taken place the parts may be covered with some antiseptic material, as carbolic acid in a watery or oily solution, one part to thirty, or with powdered chloral. When the line of demarcation has formed and the gangrenous part can be removed by amputation, such an operation may be performed.
Causes.—Though occasionally sporadic it is essentially an endemic disease in cold and damp countries, as in the deep valleys of the Alps, the Pyrenees, the Cordilleras in our own country, the chalky districts of Derbyshire in England, and so forth.
Symptoms.—A simple goitre appears to be a local affection, with only symptoms such as dyspnoea, or the cough as of a broken-winded horse on exertion, and even difficulty of breathing on the slightest cause. Whereas the exophthalmic form is part of a more general disease marked by the enlargement of the thyroid body, prominence of the eyeballs, palpitation of the heart, a peculiar thrill in the blood-vessels and a general want of muscular and brain power.
Treatment.—Simple goitres are to be treated on ordinary principles, viz., by attention to the general health, the inhalation of fresh air and by tonic medicines. Filtered or distilled water should always be taken, more particularly in districts where chalk, lime and magnesia abound. Iodine has always been held in high repute in this disease, in the form of iodide of potassium, and in four or five grain doses, given with bark or quinine, this drug is of use. For some years we have employed tonics alone by the mouth, and have ordered the air in the room to be kept iodized by means of solid iodine put into a box with a perforated lid; the metal thus evaporates steadily into the room where the patient sits and sleeps, and in this way it becomes absorbed. Under its influence we have often been surprised to find how rapidly goitres disappear. With this treatment we sometimes rub in an ointment of the iodide of ammonium, a drachm to an ounce.
|
|
|
|
|
|
|
Causes.—A low form of inflammation of the arterial walls is without doubt the most common predisposing cause, while over-action of the heart and circulation is the exciting one. Direct injury to an artery (traumatic) is an occasional cause.
Symptoms.—The early symptoms of aneurism are very uncertain. It often happens that the patient's attention is first directed to some swelling, although it may be only that of local throbbing, some weakness or stiffness of an extremity, or some nerve pain preceding the discovery of the disease; yet such symptoms are not constant. When, however, you are consulted for pain which shoots down the course of a nerve running in contact with a large artery, you should allow the thought of aneurismal pressure to pass through your mind, and, when this is associated with the presence of a tumor connected with the vessels, the suspicion of its being aneurismal should be excited. If this tumor be soft and pulsating, and becomes tense on the application of pressure to the trunk of the artery on the distal side, and placid, non-pulsatile and vanishing on pressure on the cardiac side, and should pressure on the tumor modify the pulse in the vessel below, the chances of its being aneurismal amount almost to a certainty. Should it expand again readily on the removal of pressure, this expansion is accompanied with a peculiar thrill on the readmission of blood into the sac, with a bellows murmur or aneurismal bruit, synchronous with the pulse.
Treatment.—The spontaneous cure of an aneurism is caused by the coagulation of the blood in the sac; how to induce this coagulation by natural processes is our aim; therefore, it is necessary to have a feeble circulation through it; for this purpose, rest in the recumbent position is an essential point of practice, and should be maintained in every case. When the force of the circulation is too strong and the powers of the patient are good, bleeding under these circumstances is not only rational but scientific. Medicines do not seem to have much influence in the coagulating process, though the acetate of lead has been found useful and iodide of potassium. The local treatment is based on similar principles, the aim being to diminish the circulation through the sac. This may be effected by the following means, viz., by compression in one of its forms of the artery above the aneurism, indirect; by compression of the aneurism itself, direct; by the Hunterian operation, viz., the application of a ligature to the artery on its cardiac side; by imitating the rare natural process of closure of the artery on its distal side by the application of a ligature, or by pressure, or by the artificial production of an embolic plug, by Fergusson's method of manipulation, and last of all it may be laid open and both ends tied. The treatment by electro-puncture, injection, and the introduction, of some foreign body into the sac may be adopted in exceptional cases.
|
|
|
|
|
|
|
Symptoms.—The most prominent symptom of an obstructed vein is edema of the parts below the obstruction, some fullness of the superficial veins, local pain and tenderness; constitutional disturbance of variable degrees of severity generally preceding. When superficial veins are involved the symptoms may be chiefly local, but in the case of deep veins constitutional disturbance is certain to accompany local action. Among the superficial veins the saphena of the leg and thigh is most commonly affected, and is often a sequelae of a varicose condition. Under these circumstances the tortuous, dilated, indurated vein becomes a marked object, set as it were in a frame of hardened inflamed skin and cellular tissue.
Treatment.—The two great indications for treatment in these cases are to favor venous circulation of the part, and to improve the general condition of the patient.
The first is attained by elevation of the limb, the foot being raised higher than the hip, and by the application of warmth. The second can be carried out by the administration of a simple nutritious diet, tonics, such as quinine, bark or iron, and stimulants carefully adjusted to the wants of the individual case.
Pain must be allayed by both local and general means, as poppy fomentations, and the internal use of sedatives. Leeching should never be resorted to, nor the use of mercury. When suppuration appears it must be dealt with on ordinary principles, but it is well, as a rule, to evacuate it as soon as it has declared itself.
Symptoms 1.—The absorbent glands with their ducts are liable to inflammation, adenitis or angeioleucitis, and this action is the result of the absorption of some septic material. It is almost always associated with a wound, punctured or open-inflamed suppurating, healing; with some point of irritation or suppuration, even a papule or pustule; with some centre from which morbific elements may be taken up. In what is called a simple wound the inflammation of the absorbents may be acute, but in poisoned it is violent and diffused. The inflammation always follows the course of the absorbents, leading from the centre of absorption toward the glands, that is, toward the body, and it never spreads backward. When it has reached the glands, the diseased action ceases to spread, that is, it expends its force upon the group of glands in which the absorbents naturally end, and does not extend through another series of absorbents to a second group. When pyemia follows or complicates the case, it may be open to question whether the poisonous fluid circulating in the lymphatics has not been allowed to pass into the blood through its usual channels, viz., through the inflamed glands onward, and set up inflammation in the tubes and glands, was taken directly into the blood through the venous channels, thus giving rise to blood-poisoning.
|
|
|
|
|
|
|
2. Pain and tenderness in some of the glands are generally early symptoms, and with these, or some following them, will be seen a band of redness varying in diameter, leading from the wound or infecting centre toward the gland. This red line may be continuous or interrupted; it may be a thin streak or a broad stripe of redness, and in some instances so radiate into the surrounding tissues as to simulate erysipelas. The whole line of redness is very painful, and with these local symptoms there will also be some febrile disturbance. The red lines follow the course of the absorbents and not of the veins.
Treatment.—When any indications of absorbent inflammation show themselves the wound or sore should be well cleansed and any collection of pus let out. The affected limb should be raised, the foot, when involved, brought higher than the hip; the hand or elbow than the shoulder, and warm poppy fomentations should be applied along the whole course of the lymphatics up to the group of glands in which they terminate. As soon as suppuration appears the abscess must be opened, whether this follows directly upon the inflammation or subsequently. A saline purge should be administered; sedatives should be given to allay pain. When suppuration has taken place tonics may be administered. In chronic cases, where induration in the track of the ducts remains, mercurial ointment and friction are sometimes valuable.
The glands without any outlet in the body are three in number, namely: the thyroid, situated in the front of the neck; the spleen, located in the left side below the heart, and the supra-renal capsules, which are placed one over each kidney, deep in the loins on either side of the spinal column. Although the functions of these organs are still undetermined, many of their diseases are well known.
|
|
|
|
|
|
|
Symptoms.—Diseases of the spleen may be acute or chronic. The acute symptoms are a sensation of cold and partial rigor, a feeling of weight, fullness and pain in the left side extending to the left shoulder, increased on pressure and coughing; thirst; some degree of nausea; dry cough with the usual symptoms of pyrexia. Wandering pains in the limbs, sometimes ending in collections of pus under the integuments of the thigh, arm, and so forth, are not uncommon in chronic splenitis. In the latter periods of the disease the debility and emaciation become very great; the complexion darkens and the appetite fails. Hectic, more or less violent, comes on with diarrhoea or vomiting of unconquerable pertinacity and blood is frequently discharged both upward and downward.
There is a simple enlargement of the spleen from mere temporary congestion, as when brought on by sudden mental emotion or by oscillations of the circulation from internal causes. In temperate climates the more permanent enlargement or hypertrophy of this organ, not being accompanied by the same violence of constitutional disease as in the latter, is usually of a passive character and is owing to relaxation of fibre. The most frequent causes of enlarged spleen are ague (ague cake) and remittent fever. The most characteristic symptoms are a sense of weight in the left side with or without evident swelling; inability to lie on the right side with ease; debility; disordered stomach; dry cough and absence of fever.
Treatment.—The indications of treatment are: first, to remove the cause; secondly, to restore the organ to its natural condition; and thirdly, to improve the general health. If ague be the exciting cause it must be combated by appropriate remedies, warm and brisk purgatives should be given once or twice a week so as to affect the upper bowels. Mercurials should be omitted. The bowels being kept more open than ordinary, the nascent irritative stage having gone by and the case being strictly passive, tonics are to be had recourse to and especially the acids with preparations of iron.
Leucocythemia.—Leucocythemia or white-cell blood is a disease of the circulating fluid often associated with enlargement of the spleen and supposed to be caused in part by the morbid condition of that organ. The great characteristic of this malady, as its name indicates, is the preponderance of white corpuscles in the blood.
Symptoms.—The general or constitutional symptoms are a slowly progressive anemia, weakness and emaciation, with incapacity for exertion, shortness of breath and digestive derangements. The bodily temperature is often somewhat raised and sometimes persistently elevated. The urine may he normal in appearance but less urea appears to he secreted in it. In the later stages there is a tendency to dropsy and to hemorrhage from various surfaces, especially the mucous membranes. The only certain mode of determining this remarkable disease is by a microscopic examination of the blood.
|
|
|
|
|
|
|
Treatment.—No specific for leucocythemia has yet been discovered. The constitution requires generous support, if not stimulation. Tincture of the chloride of iron in doses of ten or fifteen drops three times a day sometimes acts admirably.
Symptoms.—Dilatation of the heart is indicated, upon physical exploration, when, with extended impulse of the heart we have dullness on percussion beyond the usual limits. If true hyperthrophy or muscular thickening be present the impulse is very forcible as well as extended. The heart-sounds are apt to be clear, though not loud, in attenuated dilatation; rather loud, but dull-toned, in enlargement with thickening. It is most often induced by valvular obstruction or regurgitation, compelling unusual and continued efforts to sustain this circulation. Sometimes, however, it is more truly idiopathic, following causes of over-action of a heart otherwise sound, thus, violent exercise, self-abuse, coffee, tobacco, alcohol, and so forth, are, with good reason in predisposed cases, accused of producing it.
Treatment.—In the treatment avoidance of such exciting causes and particularly of violent exercise, alcohol and venery, is the main principle. Robust or plethoric patients may bear and be benefited by occasional leeching or cupping over the heart. Acetate of lead as an astringent cardiac sedative has proved useful in the dose of one grain thrice daily, with care to avoid saturnine poisoning. Digitalis here acts as a tonic to the heart, through ganglionic influences, lessening rapidity of action when that depends on debility, and veratrum viride as a sedative and palliative in violent acceleration of the pulse, as in muscular hypertrophy and in some forms of palpitation.
Symptoms.—Enlargement of the heart and its extent are easily determined by means of physical signs, palpation and percussion. By the touch it is found that the apex beat is more or less lowered and carried to the left of its normal situation. Between the apex and the base of the organ are found impulses not perceptible in health. By percussion the boundaries of the organ are readily ascertained in the great majority of cases. The vocal resonance also, as heard with the stethoscope, enables the physician to define the limits to which the organ extends. Palpation and auscultation furnish signs by which predominant hypertropy may be differentiated from dilatation. If hypertrophy predominates the impulses of the heart as felt by the hand are strong, and often there is a heaving movement extending over the region of the heart. The first sound of the heart, over the apex, is abnormally loud, long and booming. On the other hand, if dilatation be considerable or great, weakness of the organ is denoted by feeble impulses and by diminished intensity, together with shortness and a valvular quantity of the first sound of the heart in the situation of the apex.
|
|
|
|
|
|
|
Treatment.—In addition to purgatives we have seen the most decided advantage result from diuretics, and not only when there was dropsy, but equally when there was none. Their mode of operation appears to be ultimately the same as that of purgatives, viz., they drain off the serous portion of the blood. We have found many patients, conscious of the benefit which they derived from this class of remedies, to be in the constant habit of taking cream of tartar, brown tea and other similar popular medicines. One patient, affected with contraction of the mitral valve to the size of an ordinary pea, by these means warded off dropsy beyond the slightest edema of the feet for ten years. When decided dropsy appears it must be combated by the most efficient diuretics, the acetate, or tartrate and nitrate of potash, squill, digitalis, spirit of nitre, ether, brome, and so forth, as no class of remedies is more variable and uncertain than this. When one fails another should be resorted to.
Diet.—The treatment consists of a highly nutritious diet, into which fatty articles should enter sparingly, together with the employment of hygienic measures and remedies designed to give tone to and to invigorate the heart.
Diagnosis.—The diagnosis of valvular disease has been rendered very complete by means of auscultation. With very rare exceptions it gives rise to adventitious sounds or murmurs, the characters of which, as regards their situation, their transmission in different directions, and their relations to the heart sounds, enable the physician not only to determine their existence but to localize them and to distinguish between those which involve obstruction and regurgitation. When valvular disease has advanced sufficiently to produce obvious symptoms referable to either obstruction or regurgitation, or to both, they will destroy life sooner or later.
|
|
|
|
|
|
|
Whether the disease of the valves be cartilaginous, osseous, or consist of vegetations, the general symptoms are the same if the degree of contraction be equal. The general symptoms are cough, copious watery expectoration, dyspnoea, orthopnoea, frightful dreams and starting from sleep. Edema of the lungs, pulmonary apoplexy, passive hemoptysis (sputa stained with dark or grumous blood), turgescence of the jugular veins, lividity of the face, anasarca, injection of almost all the mucous membranes, passive hemorrhages, especially of the mucous membranes, engorgement of the liver, spleen, and so forth, and congestion of the brain with symptoms of oppression, sometimes amounting to apoplexy.
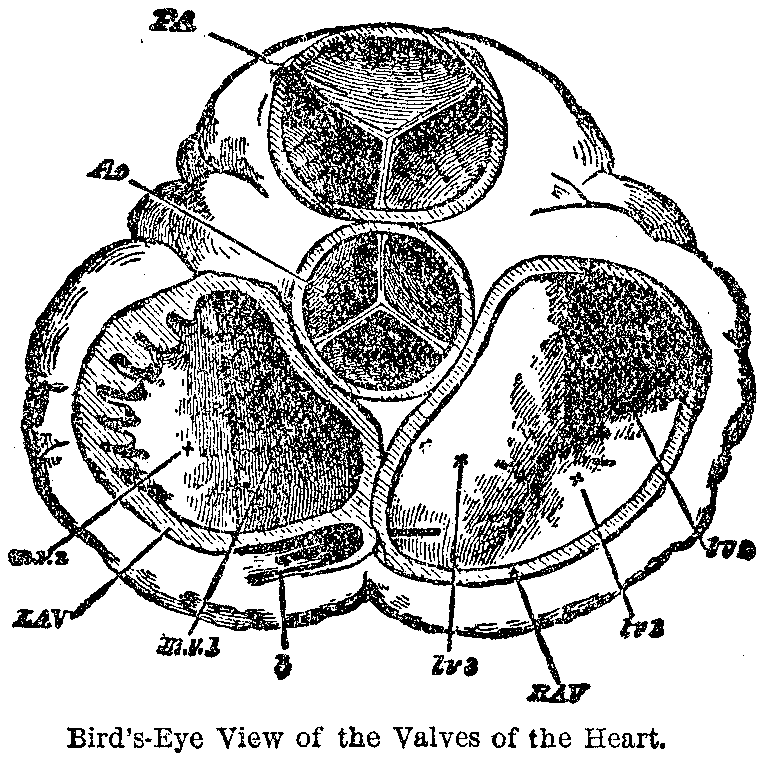
The accompanying illustration represents a hardened section of the heart, cut transversely across the organ so as to show how the pocket-like valves come together in the middle of the openings in order to close those orifices. At LAV are seen the two flaps of the mitral valve, which shuts off the return current of the blood as it is being driven by the strong left ventricle into the aorta, and at Ao are depicted the three flaps of the aortic valve, which is closed by the return current of the blood from the great aorta after it is pumped into that large blood-vessel by the ventricular contraction. It is plain to be seen that if the edges of these valves are rough or ragged or perforated, they cannot shut tightly and will allow some leakage to occur.
Symptoms.—When the disease is combined with hypertrophy or dilatation, as is commonly the case, the symptoms are more severe than those of hypertrophy or of dilatation alone, the paroxysms of palpitation and dyspnoea in particular being more violent, more obstinate and more easily excited. The action of the heart is irregular. The pulse is small, weak, intermittent, irregular and unequal.
Treatment.—Since we can neither replace or repair the damaged valves of the heart, the principles of treatment for chronic valvular disease are, in general terms, such as diminish the force and activity of the circulation, occasional venesection to a moderate extent, an unstimulating and rather spare, though sufficiently nutritious diet, a tranquil life, with respect both to the body and the mind, and a good state of the digestive organs and alimentary canal.
|
|
|
|
|
|
|
When there is dropsy diuretics are of the greatest utility. They are remarkably beneficial in an anterior stage of the disease; for, by drawing off the serous portion of the blood, they diminish the quantity without deteriorating the quality of the fluid, and thus relieve palpitation and dyspnoea and obviate infiltration, without materially reducing the patient.
When diuretics do not remove dropsy and purgatives have failed, the practitioner is compelled to resort to puncturing. We say compelled, because the remedy is a last and dangerous resource. The danger, however, may be considerably diminished by making small punctures with a grooved needle, and allowing the fluid to ooze slowly during four or five days or a week. When incisions are made with a scalpel or lance, the fluid is evacuated quickly, as in twelve or forty hours, and the patient, according to our observation, generally dies.
Complete and, commonly, sudden loss of sensation and motion with considerable diminution or entire suspension of the pulsations of the heart and respiratory movements.
Symptoms.—It is to be distinguished from an epileptic or apoplectic fit by the fuller and apparent failure of the pulse and respiration, as well as by the previous history, if that can be obtained from friends or bystanders.
Treatment.—Syncope is, commonly, an affection of no consequence, but sometimes it is an index of diseased heart. Generally, recovery from a swoon is rapid if the patient is laid flat upon the ground, without any pillow, the clothing loosened from the neck and a little cold water sprinkled in the face and the application of volatile substances to the nostrils are all that will be required during the fit. If recovery is delayed a turpentine injection or one containing a little whiskey and water should be administered, and the electro-magnetic current may be transmitted through the walls of the chest to stimulate the failing powers of the lungs and heart.
Symptoms.—All excessive or consciously disturbed action of the heart is commonly thus designated. Over-action in particular may have either of the following origins: Nervous or hysterical, dyspeptic, rheumatic or gouty, hypertrophic.
|
|
|
|
|
|
|
All of the above forms of merely functional disturbance of the heart, and especially the purely nervous, may be known from hypertrophic over-action, or the conscious impulse of dilatation of the heart, by the fact that they are not increased by moderate exercise; are often, indeed, much diminished thereby.
Treatment.—The treatment must vary according to its cause. If nervous, invigoration of the system and enrichment of the blood are most probably required, by iron and other tonics and regimen. Dyspepsia will require appropriate treatment; as a part of which exercise in the open air will not be counter-indicated at all by sympathetic palpitation.
Symptoms.—It is a disease of an intermitting character in which the patient has intervals of comparative ease or perfect health between paroxysms of greater or less suffering. It is characterized by sudden attacks of severe pain, extending from the heart along the left arm, with a sense of stricture in the chest, prostration and alarm. The pain is rarely confined to its primary and principal site in the cardiac region, but increases, in different instances, very variously both in direction and extent. It shoots upward or downward or to the right side and almost always through the left side of the chest toward the shoulder and axilla and very frequently into the left arm.
Treatment.—The violence of the patient's sufferings and the belief in the nervous or spasmodic nature of the pain, suggested by its sudden invasion, would naturally lead the medical attendant, in the first place, to attempt to afford relief by anodynes; such attempts, however, have generally been attended with less success than might have been expected. In angina, as in toothache or tic douleureux, gastralgia, colic, or other violent pains, nature seems as if she scorned to be controlled by art, although so much under the influence of similar applications when less needed, as in the case of milder pains. Antispasmodics, cordials, carminatives, and so forth, have been much recommended and employed; and, upon the whole, with better success than anodynes. The inhalation of one or two drops of nitrate of amyl sometimes relaxes the spasm and affords prompt relief. Small doses of nitro-glycerine and hypodermic injections of from one-eighth to one-half grain of morphia also partly relieve the pain after a little longer delay. But although these or other means may afford relief, or may even ward off death, it is evident that every kind of treatment confined to the paroxysm is of very slight importance. Compared with that which is to be employed in the interval, the former can, at most, afford temporary relief; the latter may cure the disease.
|
|
|
|
|
|
|
Symptoms.—Asthma from disease of the heart often imitates the characters of the other varieties, and this perhaps for a very simple reason; that the lungs are in much the same state as in those varieties. Thus the asthma is humid or humeral when there is permanent engorgement of the lungs, causing copious sero-mucous effusion into the air passages, as in cases of contraction of the mitral valve. It is dry when the engorgement is only transitory, as in cases of pure hypertrophy. It is continued when there is a permanent obstruction to the circulation, and may be convulsive when the heart has sufficient power to palpitate violently.
Treatment.—Numberless remedies have been tried; among them stramonium, nitrate of amyl, chloroform inhalations, and so forth. Arsenic enjoys full favor and deservedly holds an important rank as a therapeutic agent.
The larger blood-vessels, both arteries and veins, are liable, like the heart itself, to various structural changes in disease, which, of course, lead to more or less serious disturbances in the circulation of the blood.
Symptoms.—Arteritis or inflammation of the substance of a blood-vessel, commonly commencing with the inner coat of the artery and extending through the whole structure of the wall of the tube, is a rare affection and scarcely ever detected before death.
Fatty and calcareous degenerations of the arteries are much more common, and consist in the deposit of fatty or chalky material in the arterial walls, generally in patches varying in size from a mere speck to an inch or more in diameter.
Treatment.—These diseases do not occur until after middle life and no satisfactory treatment has been found.
This page is maintained by
Charles Keith.
Contact:
Send me a message
Last Modified: Monday, 13-May-2013 15:31:46 EDT