|
|
|
|
|
|
|
Proneness of Children to Certain Diseases.—While the diseases incident to those between three and fifteen years of age, which constitutes the period of childhood, are not confined exclusively to this time of life, and while there are few, if any, which may not occur also among infants or adults, children are particularly prone to the development of certain ailments which are rarely seen among those either older or younger. Many of the acute infectious diseases, such as scarlet fever, measles and chicken-pox belong more especially to this period, first, because children seem particularly susceptible to them; and, second, because, as they reach an age when they begin to mingle with others, they become liable to exposure to contagion, and having once had them they become, as a rule, immune, or free from liability to their recurrence, from the well-known fact that most of these diseases generally occur only once in a lifetime.
As these constitute a large proportion of what are ordinarily known as children's diseases it will be appropriate to consider them first.
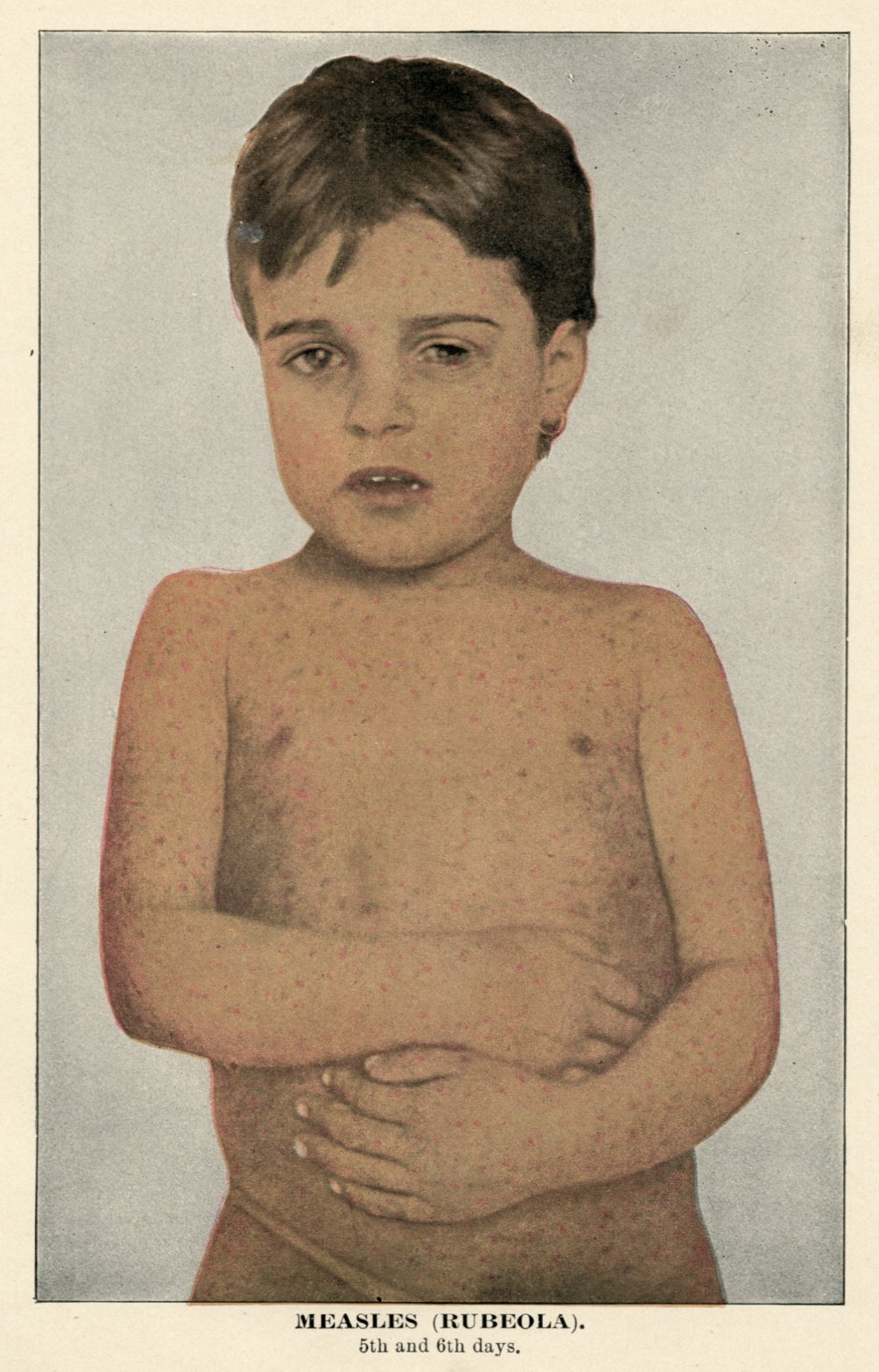
General Description.—This disease, known also as morbilli and rubeola, is highly contagious, being conveyed not only by the touch and breath of the one affected, but also by infected articles and by a third person. Of all the contagious diseases it is the most liable to recur, there being sometimes, though not often, several attacks in the same person.
Characteristics.—It is characterized by fever, catarrhal symptoms and an eruption. Unless complicated by more serious ailments, such as bronchitis, which is the most frequent, it is rarely fatal if malignant forms such as hemorrhagic and black measles be excepted. From ten to twenty days elapse after exposure to contagion before the symptoms develop.
|
|
|
|
|
|
|
Symptoms.—The ordinary symptoms of a cold in the head, with feverishness and often headache and nausea are usually first noticed, being accompanied or soon followed by cough. These persist with increasing fever until, usually on the fourth day, an eruption appears, beginning on the forehead, neck and face, and during the next twenty-four hours gradually extending over the entire surface of the body. It consists first of distinct, slightly raised red spots resembling flea-bites, which disappear momentarily on pressure; they gradually increase in size and sometimes join each other, becoming confluent and making continuous patches of dusky redness, between which healthy skin may be seen.
An entire day before the eruption appears, examination of the inner surface of the cheeks will reveal the presence of bluish-white spots.
Length of Eruption.—The eruption remains at its height only about a day, when it begins to fade, and in two or three days it has entirely disappeared. To a less extent than in scarlet fever, desquamation of a fine branny character follows, more especially when the eruption has been intense.
Temperature.—The temperature, which during the first few days continues to rise, gradually declines when the eruption appears.
Swollen Glands.—At the height of the disease the glands of the neck and the features are swollen, and the eyes are sensitive to light and affected with a profuse watery discharge which may become thicker.
Diagnosis.—Measles may be mistaken for scarlet fever and for German measles. Its rash, however, is more blotchy and less uniform than that of the other diseases and does not appear as early as does that of scarlet fever. The catarrhal symptoms are more pronounced, while in scarlet fever sore throat is a prominent feature.
Treatment.—1. For the fever, from five to ten drops of sweet spirits of nitre in a teaspoonful of solution of acetate of ammonium, or simply in sweetened water, every two or three hours, will not only reduce the temperature but act on the skin and kidneys.
2. If a laxative is needed give a half wineglassful of citrate of magnesia every half hour until the desired effect is produced. Or give one-twelfth of a grain of calomel every hour. This will be helpful also in settling the stomach if it is irritable, especially if combined with two grains of bicarbonate of soda.
|
|
|
|
|
|
|
3. For diarrhoea, which sometimes occurs, give a teaspoonful of chalk mixture every two or three hours, with five or ten drops of paregoric and two or three grains of subnitrate of bismuth.
4. For the inflamed eyes, bathe them with tepid water and drop into them every hour or two a few drops of a solution of twenty grains each of borax and boric acid and an ounce each of rose water and camphor water. The surface of the eyeball may be thoroughly cleansed with this solution, by gently separating the lids with the thumb and forefinger of the left hand and carefully expressing a medicine dropper full of the liquid into the corner of the eye. Before using it the liquid should invariably be made lukewarm by immersing the bottle containing it in a vessel of warm water for a few minutes.
5. The cough will be relieved by freely drinking flaxseed tea, with a little sugar and lemon juice, or by a half teaspoonful of brown mixture given every two hours. Camphorated oil may be applied to the chest every few hours, and a thin sheet of cotton wrapped around the chest to protect from liability to cold. If persistent, the cough may be benefited by the following, given in doses of a teaspoonful every two or three hours to a child from five to ten years old:
LATIN. ENGLISH.
Rx.---Ammonii carbonat... 16 grains Carbonate of ammonium.... 16 grains
Ammonii chloridi... 24 " Chloride of ammonium. ... 24 "
Syr. pruni virginiam, Syrup of wild cherry enough
q. s. ad........ 3 fluid ounces to make.................. 3 ounces
6. During convalescence it is advisable to give some such reconstructive and tonic as syrup or solution of hypophosphites, a teaspoonful three times daily, or a like amount of a good extract of malt, with or without cod-liver oil. This will aid in the prevention of serious constitutional and pulmonary ailments which sometimes occur as sequels of this disease.
Nursing.—The patient should be kept in bed and protected from exposure to cold, as the chief danger is from liability to bronchitis and pneumonia. Bathing the body with lukewarm water every few hours, uncovering only a small portion of the surface at a time, will add to comfort and aid in reducing fever. The room should be kept darkened on account of the condition of the eyes. When the eruption appears to be delayed or does not come out well, warm baths and hot drinks should be employed.
Diet.—Plain, simple, nutritious diet, such as is suited to all fever cases, should be given. Milk and broths will be found useful as a foundation for other articles of food.
|
|
|
|
|
|
|
General Description.—German or French, measles, known also as rötheln and rubella, is a contagious disease, usually mild in character, having as its main features fever and eruption. It resembles in some respects genuine measles. After exposure to contagion, from ten to twelve days elapse before the symptoms develop.
Symptoms.—Frequently the first symptom, and always early in the course of the disease, is the appearance of an eruption on the face, which during the first day spreads to the body and extremities. It consists of reddish spots, rather brighter than those of measles, which like those in that disease are somewhat raised and disappear on pressure. In the course of two or three days it fades away and is followed by slight branny desquamation. Accompanying this are slight fever and mild catarrhal symptoms, with quite frequently swelling of the glands of the neck.
Diagnosis.—The diagnostic points to be observed are sufficiently noted in the section on measles to which the reader is referred.
Treatment.—Rarely is more treatment needed than the spirits of nitre, recommended for the fever of measles, and for the itching of the skin, which is sometimes an annoying symptom, the surface may be dusted with compound stearate of zinc with menthol.
Nursing and Diet of a special character is not needed.

General Description.—Scarlet fever is one of the most serious of the acute infectious diseases of childhood, and [i]s characterized by fever, eruption and sore throat. It is known, also as scarlatina, a term often erroneously understood to mean a mild form of the disease. Though distinctly contagious it is not so markedly so as measles, but infected articles of clothing, and so forth, retain the power to convey the disease for long periods of time. One attack generally protects from another, although exceptions to this rule occur. From three to twelve days, and sometimes more, elapse after exposure to contagion before the disease develops.
Symptoms.—These are usually sudden in their onset. The child previously apparently well or merely languid is without assignable cause seized with vomiting or has a chill. High fever, with the temperature ranging from 103 degrees to 105 degrees, rapidly supervenes, the face is flushed, the throat is inflamed and dry, the head aches and the tongue is somewhat coated, with red points projecting above the surrounding surface, somewhat resembling a strawberry in appearance.
|
|
|
|
|
|
|
Usually on the following day a scarlet eruption appears, first on the chest, and extending rapidly over the body, being most marked in the flexures of the joints and where the surface of the skin is particularly subjected to pressure or heat. This redness may be quite uniform or may occur in patches, with intervening areas of healthy skin. On drawing the fingers quickly over the surface a white line appears, which is, however, replaced almost at once by the original efflorescence. On this red base are to be seen many distinct, bright, minute red points, and occasionally larger red spots. The inflamed surface occasions itching of varying intensity and swelling of the skin. In the course of two or three days the eruption gradually fades, and with this the temperature declines. The outer layer of the skin now gradually peals[sic] off in flakes of variable size, the palms of the hands and the soles of the feet usually being the last to undergo this process. Until this has entirely ceased, and it may be prolonged to six or eight weeks, the danger of conveying the disease persists, inasmuch as the source of contagion lies largely, though not exclusively, in these particles of skin.
Prominent Features of the Disease.—Among the most pronounced features of the disease are the swollen glands of the neck and the inflamed condition of the throat, which may be so marked as to produce patches resembling those seen in diphtheria. These consist of a membranous exudate which sometimes extends from the throat into the adjacent passages, causing serious complications. Among these is inflammation of the middle ear, with perforation of the ear drum, one of the most frequent causes of deafness. Frequently the kidneys become involved, acute inflammation of greater or less intensity occurring. Recovery from this, however, is usual.
Convulsions.—Convulsions may be present either from the kidney complications or from profound impression on the nervous system by the poison of the disease In the latter cases the disease assumes a malignant type, with excessive temperature, delirium, stupor and often diarrhoea and vomiting, as symptoms which rapidly lead to a fatal issue, sometimes within a few hours. On the other hand cases occur which are so mild as to be scarcely recognizable as genuine scarlet fever, except from observation of a sequel and inquiry as to preceding circumstances. A physician, for instance, may be consulted for edema or dropsy of the extremities, indicating the existence of kidney affection, and on investigation may ascertain that a few weeks before the child had had a slight rash, followed by desquamation, without complaining sufficiently to be kept in bed, and that there is a history of its having been exposed to the contagion. Such a record would justify the diagnosis of scarlet fever.
|
|
|
|
|
|
|
Irregular Manifestations.—Besides these variations from the usual type of the disease there are irregular manifestations, such as the hemorrhagic form, and grave complications such as gangrene and heart disease, which cannot, however, within the limits of this article, receive more than passing mention.
Diagnosis.—1. Acute exfoliative dermatitis is a disease of the skin in which marked desquamation occurs, resembling in this particular scarlet fever. The throat symptoms, however, so significant of the latter disease, rarely occur, nor is the characteristic appearance of the tongue present.
2. Measles.—The throat symptoms instead of the catarrhal manifestations; the sudden onset instead of the gradual development; the character of the eruption and the fact that it appears much earlier in scarlet fever, and the difference in the temperature record usually suffice to enable a diagnosis without much difficulty.
3. German Measles.—This has already been discussed in connection with that disease.
4. Diphtheria.—From this disease it differs, in that the false membrane in the throat does not appear for a number of days after the beginning of the illness, whereas in diphtheria it is seen at once. The early appearance and the characteristics of the eruption are also diagnostic points of value.
Nursing.—A warm bath at the outset of the disease will promote the activity of the skin and aid in bringing out the eruption. Frequent sponging with lukewarm water throughout the attack is of advantage. When desquamation begins the surface of the body should daily be anointed with carbolized vaseline or other ointment oil to facilitate the process of scaling and to aid in preventing the small particles from becoming scattered. Particular care should be exercised to gather all these and burn them. In order that all may be obtained a large sheet should be spread on the floor beneath the bed. The utmost caution should be observed to prevent the patient from taking cold, both during the attack and after convalescence is established, and for fully a week after the temperature is normal he should still be kept in bed.
Diet.—Milk, broths and water may be freely given, and if the fever is high ice bags may be advantageously applied to the head.
Treatment.—1. For the throat symptoms, a spray of peroxide of hydrogen and water, equal parts, should be used; or a saturated solution of chlorate of potash may be employed as a gargle. Cold applications to the neck are also useful.
|
|
|
|
|
|
|
2. In severe cases stimulants may be required for the weak condition of the heart. Half teaspoonful doses of whiskey, or ten-drop doses of aromatic spirits of ammonia in water should in these cases be given every two hours. Drop doses of tincture of digitalis every three hours are also useful.
3. In case the inflammation extends from the throat and involves, as it often does, the ear, the aid of a specialist in ear troubles will probably be required to save the patient from impairment of hearing.
4. In inflammation of the kidneys, five grains of acetate of potash and a teaspoonful of infusion of digitalis every three hours will be proper for a child five years of age.
5. The following is useful for the reduction of fever:
Tincture of aconite............................. 20 minims
Solution of citrate of potash.................... 3 ounces
Give a teaspoonful in a little sweetened water every hour until the fever is reduced and the skin becomes moist.
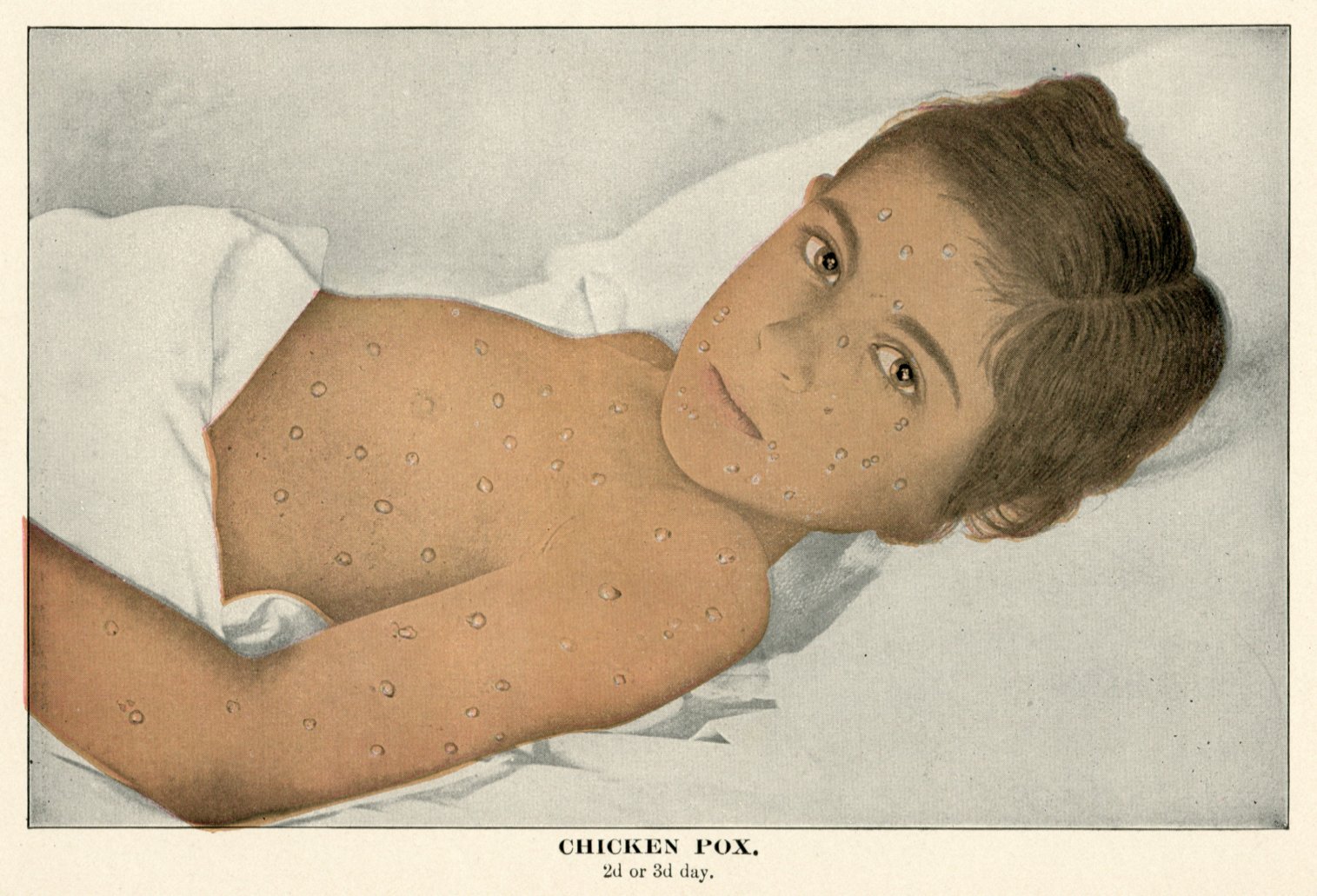
General Consideration.—Chicken-pox or varicella is a contagious disease having an eruption of vesicles. It generally occurs in children under six years of age, though it is sometimes seen in adults. One attack confers immunity from a recurrence in the same individual. From ten to seventeen days elapse after exposure to the contagion before the symptoms develop.
Symptoms.—Often the appearance of the eruption is the most marked symptom, although there is also slight fever which may be accompanied by chills, vomiting, headache and pain in the back and legs. The eruption comes out during the first day, usually appearing first on the chest or back, though sometimes on the forehead in the form of red spots. Later they are seen also on the extremities. They vary in number from one or two dozen to several hundred.
In the course of a few hours the papular spots become vesicular, filled with a turbid liquid, and these by the end of a day or so begin to dry. Fresh crops during the few days following continue to appear so that by the third or fourth day they may be seen in all stages of development. Itching is often quite marked, and scars are apt to result if the patient is not prevented from scratching.
|
|
|
|
|
|
|
Diagnosis.—Failure to distinguish this disease from mild cases of small-pox has not unfrequently occurred. In the latter disease, however, the eruption does not appear until the third or fourth day of the disease, and it is first seen on the face and forehead. The vesicles are not present until the fifth or sixth day; they become depressed in the centre and by the eighth day become pustular, not beginning to dry until after this time. The eruption is not seen in different stages of development as in chicken-pox. It is quite frequent in small-pox also to observe in the beginning of the attacks rashes resembling those of scarlet fever and measles.
Nursing and Treatment.—A mild laxative and a simple fever remedy are all that are required. Five drops of sweet spirits of nitre in a little water every hour, if the fever is marked, will be sufficient. Most cases require no treatment except isolation.
The following contagious diseases differ from those already considered, in the fact that they occur without eruption, namely, diphtheria, whooping-cough and mumps.
General Consideration.—This is a highly contagious constitutional disease, having a local manifestation in the form of a false membrane, which occurs either on the skin, or, more often, on the mucous membrane. Its usual locations are the throat, nose and larynx. The disease may be very mild or it may be extremely fatal. Different epidemics exhibit different degrees of virulence, and the cases occurring early in a given epidemic are usually the most severe. It is communicated by inoculation, by contact with the person affected, by means of the saliva, the pharyngeal secretions and portions of membrane; by exposure to the poison of the disease through the agency of infected clothing, bedding, apartments, and so forth, and through foul emanations. Defective sanitary conditions favor its development. Its occurrence is associated with the presence of a certain special germ which is supposed to be the cause of the disease. In some cases, however, the germ cannot be found; in others it is seen only early or only late in the disease; while again the germ may be found in the throats of those who present no constitutional or local symptoms of the affection. One attack does not confer immunity from another attack, and the symptoms develop from two to twelve days after exposure to the contagion.
Symptoms.—The initial symptoms are those ordinarily attending a slight cold, such as a feeling of fullness and irritation of the throat, accompanied by moderate fever, chilliness and general lassitude. Although it may be delayed for a day or two, usually within a few hours, examination of the throat reveals on the tonsils the presence of a small whitish-gray patch or patches of fibrinous exudate or false membrane, which spread with greater or less rapidity, often involving the pharynx and nose, and Extending downward to the larynx, and so forth. The color soon becomes dirty gray or yellowish. If the membrane is removed new membrane rapidly forms in its place. With the progress of the case, if it is severe, the constitutional symptoms become more marked; the glands of the neck swell; delirium and stupor may occur; the heart becomes weak and there is every indication of profound blood poisoning. This may indeed be manifested quite early in the course of the disease. With these grave symptoms it is not infrequent for the temperature to be but slightly raised or even subnormal. The presence of a thick membrane is not necessarily indicative of the existence of a grave case, for severe symptoms are quite as apt to occur when the membrane is thin. There may be considerable destruction of tissue from the sloughing membrane giving rise to intense fetor.
|
|
|
|
|
|
|
When the membrane involves the larynx an additional element of danger confronts the patient in the mechanical obstruction of the air passages. The breathing is harsh and rasping, the voice often suppressed to a whisper, a brazen, croupy cough develops, pallor of the countenance and lividity of the lips may supervene, the patient struggles for air and unless speedily relieved death from suffocation occurs.
In the milder cases of tonsillar and pharyngeal diphtheria, after persisting for a few days, the membrane gradually disappears, coincident with which there is decided amelioration in the symptoms. Even in mild cases, paralysis of the muscles of the throat is quite apt to occur, causing difficulty in swallowing liquids, which often regurgitate through the nose. Renal complications sometimes occur.
Diagnosis.—1. Tonsillitis. In mild cases of diphtheria affecting the tonsils alone, it is difficult and sometimes impossible to distinguish them from cases of tonsillitis with exudation. As a rule, however, the thickness and gray color of the membrane, its tendency to spread, the glandular involvement and the general severity of the symptoms in diphtheria simplify the matter of diagnosis. The presence of the Klebs-Loeffler bacillus, the germ already alluded to, may be taken as confirmatory evidence of the disease.
2. Membranous Croup.—In the present state of knowledge it does not seem possible to differentiate with absolute certainty between membraneous croup which is non-infectious in character and which is probably relatively infrequent, and diphtheria affecting the larynx. The absence of constitutional symptoms and of local manifestations of diphtheria elsewhere, and inability to demonstrate the presence of the germ in portions of expectorated membrane are presumptive evidence of the non-contagiousness of the attack.
|
|
|
|
|
|
|
3. Scarlet Fever.—Cases of diphtheria sometimes occur in which there is an erythematous rash which may lead to confusion in diagnosing them from scarlet fever. For the points of distinction the reader is referred to the article on the latter disease.
Nursing.—The air of the room should be kept warm and moist, especially where there is a tendency to laryngeal involvement. Fresh air should be freely admitted and disinfectants employed to keep it pure. Pieces of ice may be allowed for the patient to suck and cold applications be made to the throat. Liquid nourishment should be systematically given.
Treatment.—1. In severe cases whiskey should be given every two or three hours in teaspoonful doses to sustain the vital forces.
2. The use of calomel and corrosive sublimate has its advocates, and while other plans of treatment are now more generally in use the benefit from their employment under suitable conditions seems incontrovertible. The writer has seen numerous cases in which the most violent symptoms, growing steadily worse, abated with surprising rapidity in response to the administration of from five to ten grains of calomel given hourly to a child until several characteristic movements of the bowels were produced. Corrosive sublimate in doses of about 1-100 grain have then been advantageously employed, i
3. The local employment of lactic acid, one drachm to three ounces of lime-water, or of pancreatic extract, pepsin or vegetable pepsin, for the purpose of dissolving the membrane is advocated by some. Inasmuch, however, as the constitutional symptoms persist in spite of the removal of membrane and as its presence is usually not a menace to the patient the advantage of the practice is not apparent. It is of benefit, however, to use antiseptics locally. Peroxide of hydrogen diluted with an equal amount of water (may be used as a spray every hour or two) or weak solutions of formalin.
4. Iron and chlorate of potash have long been used, both for their local effect and their constitutional action. A mixture of this sort is of benefit:
|
|
|
|
|
|
|
Tincture of chloride of iron................... 1-1/2 drachms
Chlorate of potash............................ 48 grains
Glycerine ..................................... 4 drachms
Water enough to make........................... 3 ounces
Dissolve, and give a teaspoonful every two hours.
5. When the larynx is involved inhalations of the vapor of lime-water, especially in combination with liquor potassae in the proportion of one drachm of the latter to one pint of the former, aid in dissolving the membrane. A blanket should be suspended over the bed in such a way as to form a tent, beneath which should be used a croup kettle or steam atomizer containing the liquid.
6. In cases which become progressively worse, and in which the signs of non-oxygenation of the blood indicate that death is imminent, tracheotomy in which the trachea is cut open, or intubation, in which, without cutting, a tube is inserted into the larynx through the mouth, will often save life if resorted to sufficiently early.
7. Tonics and reconstructives are needed in convalescence, and quinine, iron, arsenic and the hypophosphites, and the use of the most nutritious foods are indicated.
8. Antitoxin. Within the last few years the use of antitoxin, both as a means of prevention and of treatment, has been warmly debated. While its enthusiasts favor its employment in every case presenting symptoms of diphtheria, without even waiting to establish a diagnosis, in case doubt as to the character of the ailment exists, the more conservative men in the profession, who still have faith in its utility and efficacy, believe that the field for its employment should probably be limited to cases which present severe symptoms and to cases which do not respond promptly to ordinary methods of treatment. To procure good results, however, the remedy should be used before the vital forces are exhausted, or the blood profoundly poisoned.
The improved methods in the manufacture of this product and its increasing reliability are fast gaining advocates for its more universal adoption.
In a child over two years of age from 1,000 to 1,500 units is the usual dose, or if the case is very severe, 2,000 units. The serum is very slowly injected beneath the skin, in the loose cellular tissue, preferably at the side of the abdomen, and allowed to be absorbed without friction. In from twelve to eighteen hours the dose is repeated if there is no improvement, and a third dose, usually of one-half the amount first used, may even be necessary. As an immunizing agent 1,000 units may be employed. The immunity conferred does not last a great while, probably less than thirty days, so that with new exposures, repeated immunization is necessary.
|
|
|
|
|
|
|
General Consideration.—Whooping-cough or pertussis is a contagious disease, mainly of childhood, characterized by catarrh of the air passages and a significant cough. It is communicable from person to person by the breath and bodily exhalations and by the agency of apartments which have become infected. It is not the harmless disease which it is so often regarded as being, for aside from the deaths which result from the disease itself, there are very many which are indirectly traceable to it, owing to complications and the after-effects of the disease.
Symptoms.—For a week or ten days these are the symptoms of an ordinary cold, with cough, slight fever, and so forth. The cough gradually increases in severity and assumes the spasmodic character which gives to the disease its name. The paroxysms consist of a series of short expulsive coughs, in which the child often becomes blue in the face and apparently on the verge of suffocation, when a long drawn noisy, whooping inspiration occurs. Thick stringy mucus is expectorated, often with vomiting, and sometimes with hemorrhages from the nose, lungs, and so forth. Several of the attacks may follow each other in close succession and then a respite of varying length occurs. After several weeks the paroxysms become less frequent and less violent, and finally cease, although for many months mild attacks may be induced by transient colds, crying, and so forth. While one attack usually confers immunity, it is frequent for other members of the family in which the disease occurs to be affected by a nervous cough, closely simulating the true disease.
Nursing.—Except in very severe cases, with complications, or where the patient becomes exhausted from loss of food, it is not necessary to confine him to the bed or the house. An abundance of fresh air is desirable, although this must be secured without exposing other children to the danger of infection.
Treatment.—1. Inhalations by means of a steam atomizer or croup kettle, of medicated steam often afford relief to the paroxysms, limiting their frequency and severity. For this purpose carbolic acid, which may be advantageously combined with an alkali is recommended, as in the following formula, used by Dr. J. Lewis Smith, late of New York, and Dr. John M. Keating, late of Philadelphia:
|
|
|
|
|
|
|
Crystallized carbolic acid ...................... 3 grains
Borax ........................................... 20 "
Bicarbonate of soda ............................. 20 "
Glycerine ....................................... 1 ounce
Water ........................................... 1 "
Some of the crude coal tar products, such as cresol, have proved markedly beneficial by inhalation.
2. Internally, belladonna has long been employed with a fair measure of success. For a child of five years, six or eight drops of the tincture should be given night and morning, until the characteristic dryness of the throat is produced.
3. Antipyrine in doses of three or four grains several times daily is often helpful, but must be given with care on account of its depressing effect on the heart.
4. Bromide of potash, from three to five grains, every three hours is useful where the nervous element of the disease is prominent.
5. Bromoform, a drop for each year of the child's age given every three or four hours, is one of the most satisfactory of the more modern remedies.
General Consideration.—Mumps, parotitis or parotiditis, is an infectious disease in which inflammation and swelling of the parotid gland occurs. Its symptoms develop from twelve to twenty-one days after exposure to the contagion. Unless complications occur, it is not a serious malady.
Symptoms.—Slight fever, swelling and tenderness of the parotid, and sometimes submaxillary and sublingual glands, with or without pain, are the main symptoms. The swelling extends both in front of and behind the ear, and eating, swallowing and even speaking may be difficult. The secretion of saliva is at times increased, at others, diminished. Either one or both sides may be affected, and in the former cases the immunity which is conferred by one attack is limited to the side which was involved. After lasting for a week or ten days, recovery rapidly takes place. Among the complications are the occurrence of orchitis and occasionally of mastitis.
Nursing.—Care should be taken to avoid exposure to cold and the patient should be fed on liquid and soft foods.
Treatment.—Nothing more than a mild laxative and a slight fever mixture is required. Either heat or cold, whichever is most comfortable, may be applied, and an ointment of ichthyol and lanoline one part to four.
|
|
|
|
|
|
|
In addition to the contagious diseases, both eruptive and non-eruptive, are several which, though not confined exclusively to children, occur so often in them as to require consideration.
General Consideration.—St. Vitus' dance, or chorea, is a disease of the nervous system, characterized by involuntary and irregular muscular movements, without consciousness being suspended. There is a marked connection between this disease and the occurrence of acute rheumatic fever or inflammatory rheumatism and of endocarditis, or inflammation of the membrane lining the heart's cavities. It more frequently is seen in those having a pronounced nervous temperament and there appears often to be a family predisposition to the disease.
Strong emotional occurrences, such as deep grief, fright, and so forth, are sometimes the exciting causes, as are also great nervous strain and mental application.
Symptoms.—Every effort of the patient to perform a voluntary muscular act is attended by irregular spasmodic movements, over which he has no control, and the stronger the effort made, the more pronounced is this condition. The symptoms generally come on gradually, though sometimes suddenly, beginning usually in the hands and arms and extending to the face and legs. One or both sides may be involved and the movements may be general or confined to a few muscles. During sleep they are rarely continued. The disease may last for a few weeks only, or may persist in spite of treatment for many months or even years. It frequently recurs, especially in the spring of the year.
Nursing.—1. Rest in bed, quiet and separation from those members of the family who are not actually engaged in taking care of the patient should be secured. The general improvement of nutrition by means of good food and tonics should be aimed at and efforts made to overcome any impairment of the digestive function. After a few days of rest, which in very severe cases may have to be obtained by gentle restraint of the active muscles, massage and carefully regulated Swedish movements will be of advantage. Spraying the spine with ether is sometimes beneficial.
|
|
|
|
|
|
|
2. Iron in assimilable form, as the peptonate, is useful. The arseniate of iron in doses of 1-100 of a grain or more three or four times a day is an eligible preparation.
3. Arsenic in the form of Fowler's solution (liquor potassae arsenitis) is more employed than any remedy. For a child of eight years five drops may be given in water three times a day after meals, and the amount increased until the constitutional effect is produced.
4. Strychnine has also been employed in many cases with good results. Beginning with a dose of 1-150 of a grain it may be increased until its physiological effects are noticeable.
General Considerations.—Incontinence of urine or eneuresis is a disease frequently occurring in children, both in acute and chronic form.
Sometimes due to malformations of the bladder it is more often caused by irritation due to too great acidity of the urine, stone in the bladder, phimosis and the presence in the rectum of worms or of a fissure. Or it may be due to weakness of the muscles of the sphincter controlling the bladder, to their being in an irritable condition, or to an excessive secretion of urine. It is the form occurring at night with which we are particularly concerned.
Treatment.—Manifestly the treatment must depend on the condition present.
1. Too great acidity is readily cured by administering liquor potassae (solution of potash) in five-drop doses every three hours in a wineglassful of water, and continuing it for a while after the urine has become neutral or alkaline in reaction.
2. Where there is too great contractile power of the muscles, belladonna should be given in five-drop doses of the tincture, at bed-time, to a child of five years, to be increased if not productive of good results until pronounced dryness of the throat occurs. If it is beneficial it may have to be continued for some time to avoid a relapse.
3. Where there is a lack of tone to the muscles, extract of nux vomica and ergot are often useful.
4. An excessive amount of urine may be controlled by limiting the fluids taken before retiring for the night.
5. The other causes of incontinence must receive their appropriate treatment.
|
|
|
|
|
|
|
General Considerations.—Several forms of worms infest the intestinal tract, the most common of which, in this country, are the "round worm," "thread worm" and "tape worm."
Round Worms.—The round worm or ascaris lumbricoids is reddish or yellowish-red in color and cylindrical in shape, with tapering extremities, resembling somewhat the ordinary earth worm. From the intestinal canal it may travel to any part of the alimentary tract, and has been found in other parts of the body. They may occur singly or in large numbers.
Thread Worms.—The thread worm, pin worn or oxyuris vermicularis is a small whitish worm inhabiting the rectum and colon.
Tape Worm.—Of tape worms there are two kinds common in man, the taenia solium or pork tape worm and the taenia saginata or beef tape worm. The latter is the larger, often being twenty or more feet in length. Its head is provided with "suckers," by means of which it adheres to the mucous membrane of the intestine; the pork worm has also hooks which it inserts and secures a firmer hold. The entire body may be cast off, yet if the head remains a new body will grow in the course of a few months to as large a size as the first. The body is composed of small flat segments, appearing like a piece of tape marked into squares or oblongs. Separate segments or continuous ribbons of segments are often passed and are for a short time endowed with slight motility.
Symptoms.—Various nervous and digestive disturbances may be produced by the presence of worms, or there may be no constitutional symptoms whatever. The thread worm causes intense itching in the rectum, especially at night.
Treatment.—1. Round Worms.—Santonin, three grains, or given in divided doses, followed by a saline laxative or a dose of calomel, is one of the most satisfactory plans of treatment. It may need to be repeated on several successive days.
2. Thread Worms.—Santonin and laxatives are also useful in treating this form of worm. Injections of quassia and water (a handful to a quart), of salt water or of carbolic acid and water (ten grains to a pint) are also advisable.
3. Tape Worm.—For two days before beginning the treatment the diet should be light, and for a full day only milk with a little bread should be allowed. A laxative should be given, and on the following day a drachm or two of the oil of male fern, preferably in capsules. This should be followed in about two hours by a dose of castor oil or of citrate of magnesia.
|
|
|
|
|
|
|
When the worm is passed careful examination should be made for the head. An infusion of pomegranate root, or its active principle pelletierine, is also one of the best remedies known. Or three or four ounces of pumpkin seeds may be bruised, soaked for twelve hours in water, and the liquid, or preferably the entire preparation, taken at once,
This page is maintained by
Charles Keith.
Contact:
Send me a message
Last Modified: Monday, 13-May-2013 15:31:46 EDT