|
|
|
|
|
|
|
The Plan and Scope of the Subject.—In this part of the work, the author proposes to give an outline of the natural history of each disease, advice as to the modes of preventing its onset when threatened, recommendations as to its hygienic management, hints as to its probable course, fatality, and ultimate results upon the system, if recovery takes place, and finally suggestions in regard to its medical treatment.
Home Value of the Book.—As already advised, the most skillful physician who can be procured should be called in to treat disease; but in the emergency, until he arrives, much can be done in accordance with the directions here given to allay the sufferings of the patient, to place him in a more favorable position for speedy recovery, and, above all, to prevent the calamity which has befallen him from becoming aggravated before the doctor comes, through want of proper care.
Manner of Treatment.—Since a large proportion of the "ills which flesh is heir to" are rarely seen in this country, and have therefore but little importance to inhabitants of the United States, except as matters of curiosity, it is proposed to give very brief notices of these infrequent maladies, in order to economize space for a fuller account of those prevalent diseases which, sometimes in their lives, will, alas, personally interest a majority of the readers of this book.
Among the almost innumerable methods of classifying diseases which afflict the human family, one of the latest, and probably the best, is that devised by the Royal College of Physicians of England, and adopted by law as the basis for all those statistical reports relating to medical subjects of which the British nation is justly entitled to be proud. This, with some unimportant variations, is the system adhered to in the present section.
|
|
|
|
|
|
|
English Names for Diseases.—The plan of this nomenclature is to give an English name to the disease, employing the terms in popular use whenever they are not absolutely inaccurate, and to use only one word, or as few words as possible, in naming a disease. Definitions are attached to the English names in certain instances only, that is in cases where there might otherwise be some ambiguity in the signification of the title. The classification of diseases thus designated is based on their anatomical seat in the human body, the division being first into general diseases and local diseases.
General Diseases.—The general diseases are those which affect the whole frame, and are subdivided into two sections. The first comprehends those disorders which appear to involve a morbid state of the blood, and for the most part present the following characteristics. They run a definite course, are attended with fever, and frequently with eruptions on the skin; are more or less readily communicable from person to person, and possess the singular and important property of generally protecting those who suffer with them from a second attack; they are apt to occur as epidemics. Small-pox is a good example of this group, and in our ceaseless combat with disease it is with disorders of this section that hygiene and preventive medicine have won their grandest triumphs and accomplished their most beneficent work.
Constitutional Diseases.—The next of the general diseases comprises for the most part maladies which are apt to invade different parts of the same body, simultaneously or in succession. These disorders are sometimes spoken of as constitutional diseases, and they often manifest a tendency to transmission by inheritance. Gout and rheumatism furnish good illustrations of this type of disease.
Diseases of the Organs.—The second class, that of local diseases, comprehends all those which affect the structure of special organs, or particular parts of the human body, leading to marked disturbance of their functions. Diseases of the eye, such as cataract, and local inflammations, such as pneumonia or inflammation of the lungs, exemplify the characters of this group. Owing to the wonderfully close association and sympathy between all the different parts of the human frame, no one organ can suffer alone, and hence with the local diseases constitutional disturbances, such as fever, generally arise, and may totally mislead an inexperienced observer.
|
|
|
|
|
|
|
Recognition of Local Diseases.—The recognition of local disease in obscure cases is often, indeed, one of the most difficult problems a physician can be called upon to solve. Commonly complaint of pain in some particular part directs attention to that spot as the seat of primary disturbance, and leads to its thorough examination, which should be made with the aid of all the mechanical appliances, such as the stethoscope, the microscope, the thermometer, and so forth, which medical science has placed at our disposal. It is only when after all these means are exhausted, in a vain effort to detect local disease at the seat of pain or of pronounced discomfort, sufficient to account for that disturbance, that we are justified in considering local distress as a mere symptom of general disease.
Complicated Diseases.—Unfortunately, neither a general nor a local disease gives the sufferer any positive security against the onset of another malady at the same time, and we often see people burdened with a complication of disorders, each of which by its symptoms obscures the rest, and perhaps renders the proper treatment for them inadmissible. It is this tendency to the development of complications, either secondary to the chief disease or entirely independent of it, which in many affections is the indirect cause of death.
Damaged Organs.—Frequently, too, after a severe illness, some important organ is damaged in its structure, and the patient for the rest of his life suffers for want of its proper performance of function throughout his whole organism, which is really as much crippled in its work as a man would be if his leg or arm had been left upon a battle-field. This is especially the case with the heart after an attack of inflammatory rheumatism, which, by affecting the cardiac valves, prevents the circulation of the blood from being duly carried on, and, as it grows worse in later years, is apt to terminate existence abruptly by sudden death, or by the painful method of prolonged and lingering illness.
Care in Dosing.—The greatest care must be exercised in portioning out the doses of medicines suggested for the treatment of the diseases described, and it should always be recollected that a mistake which is a mere blunder in other vocations may at any moment become a crime in the occupations of prescribing, preparing, or administering medicines. Hence the doctor, the apothecary, and the nurse, who have always the life of the patient in their keeping, should be persons who are willing and able to fully realize their responsibility; those who, whilst on duty, are unceasingly and vigilantly on guard against committing an error of any kind.
Doses Are Always for Adults.—The doses of medicines recommended in this section of the work are always for adults, unless otherwise expressly stated, and must be proportionately reduced for children according to age. Thus, for a young person of from fourteen to sixteen years, two-thirds of the ordinary dose should be given; from ten to thirteen, about one-half; from eight to ten, two-fifths; from six to eight, one third; for a child of four or five years, one-fourth; for one of three years, one-fifth; for one of two years, one-seventh; for an infant of one year, one-thirteenth; and for a baby of from three to six months, one twenty-fourth.
|
|
|
|
|
|
|
Doses for Children.—For example, the average dose of bromide of potassium for a grown person being twenty grains, that for a youth between fourteen and sixteen years would be sixteen grains; between ten and thirteen, ten grains; between eight and ten, eight grains; between six and eight, seven grains; between four and five, five grains; at three years, four grains; at two years, three grains; at one year, a grain and a half; and at six months, three-quarters of a grain.
How to Graduate Doses.—These fractional amounts are most conveniently arranged for young children by diluting a single dose for an adult with the requisite number of teaspoonfuls of pure water. That is to say, using the above illustration, if it is desired to administer bromide of potassium to a child one year old threatened with convulsions, twenty grains of the drug might be dissolved in thirteen teaspoonfuls of water, and a teaspoonful given every hour or two.
Why Doses Should Vary.—The doses of medicines vary, as already pointed out in the earlier part of this volume, in accordance with sex, idiosyncrasy and habit, and one of the most important advantages enjoyed by a skilled family physician is his power, gained by long practical experience, of so adapting each dose of medicine to every individual of a family, as to gain the greatest amount of benefit with the least amount of injury in any particular case.
Opiates and Emetics.—The general rule given above in regard to doses of medicines to children has some exceptions, the most important being in regard to opium, which is not well borne in childhood, and calomel or castor-oil, of which a larger proportionate quantity may be administered. In regard to the frequency of repetition of medicines, it should be understood that when not otherwise stated, this may be judged of by the effect produced. Thus, as a rule, an emetic may be repeated in fifteen minutes if the patient does not vomit; an opiate may be repeated in an hour if pain still continues without mitigation, and a cathartic in from six to eight hours if no purgative action is effected.
Change of Medicines.—In those unfortunate patients who cannot take laudanum, morphia, or paregoric for the relief of pain, which constitutes the great symptom of disease, codeia, chloral, hyoscyamus, bromide of potassium, Indian hemp, and lactucarium may be used as substitutes, but without much expectation that they will fully serve the purpose of opium, that greatest boon to suffering humanity.
|
|
|
|
|
|
|
Definition.—An acute and highly contagious disease characterized (a) by an eruption, which by the third day is papular, by the sixth day is vesicular and by the ninth it becomes pustular (b) by a fever which appears with the onset, disappears with the eruption, but returns again when the eruption becomes pustular.
History.—Small-pox was first accurately described by Rhazes, an Arabian physician, in the ninth century, and distinguished by him from measles, but it is believed to be the same as the pesta magna described by Galen (A. D. 130-200). It is known to have prevailed during the sixth century and again about the time of the Crusades. The disease is believed to have been introduced into America by the Spaniards early in the sixteenth century.
Cause.—Small-pox is one of the most virulent of the contagious diseases, the poison of which is extremely tenacious of life; it may remain latent in clothes for a long time, and then be capable of exciting the disease. The contagion exists in the secretions and excretions, and in the exhalations from the lungs and skin. The dried scales constitute by far the most important element, becoming attached to clothing and furniture; and are conveyed by persons who have been in contact with the sick. The disease is probably contagious from a very early stage, though it has not yet been determined whether the contagion is active before the eruption develops. The degree of mildness or severity of a case does not influence that of another caused by it, the severest cases being at times followed by the mildest forms, and vice versa.
Age.—Unless protected by vaccination or a previous attack, nearly every one is susceptible, from the aged to the child in the womb. The disease is usually fatal in the very young.
Sex.—Male and female are equally affected.
Race.—The North American Indian and the negro are particularly susceptible to it.
|
|
|
|
|
|
|
Nature of the Disease.—The eruption consists in an infiltration of cells into the rete mucosum or into the true skin. Genuine pock marks are frequently found in the mouth, esophagus and larynx and there are parenchymatous or soft cellular tissue degenerations in other organs.
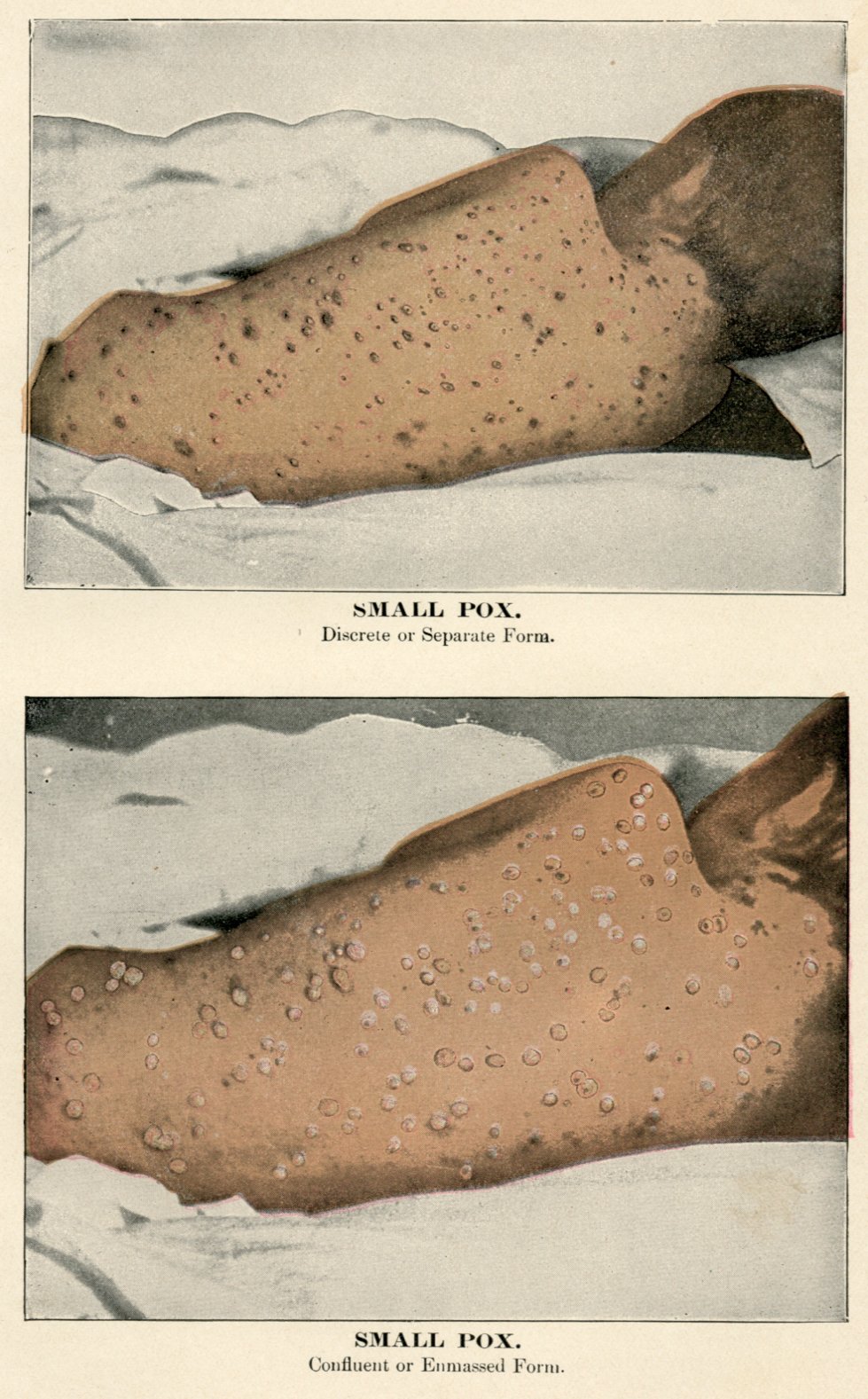
Varieties.—Discrete, confluent, malignant and varioloid.
Symptoms.—1st. Discrete form: After a period of incubation of from nine to fifteen days (Osler), seven to twelve days (Tyson), the disease is ushered in with a chill in adults, and with a convulsion in children. There is an intense frontal headache and agonizing lumbar pains, and vomiting. The pains in the limbs and back are more severe in the initial stage of this than of any other eruptive fever, and connected with the frontal headache and vomiting are specially and decisively characteristic, or pathognomonic, of this disease.
Fever sets in rapidly and may go as high as 103 or 104 the first day; the pulse is rapid, hard and strong at this stage. Delirium may be present, and is at times violent. The face is flushed and the eyes are bright and clear.
The Eruption.—About the third or fourth day small red spots are noticed, first on the forehead and wrists, from which it rapidly spreads over the face and extremities. At this stage the eruption is not unlike measles, but in another twenty-four hours it is quite different, the papules having a "shot like feeling," from which stage they pass into the other two stages mentioned in the definition. As the eruption comes out the fever falls, symptoms abate and the patient feels more comfortable. On the fifth or sixth days the papules become converted in the vesicles, which contains a clear fluid, the vesicle itself having a depressed or umbilicated centre. By the eighth or ninth day the vesicles are converted into pustules, the umbilication disappears and the fluid becomes a grayish yellow, owing to the contained pus. At this stage the fever rises and the general symptoms return. In the discrete form the fever does not usually remain high for more than twenty-four or twenty-six hours, so that on the tenth or eleventh day the fever disappears and convalescence sets in. By the fourteenth day the pustules become dry, are converted into crusts and drop off, leaving, in mild cases, a simple discoloration which in time disappears, but in severe cases a more or less deep ulcer, or, if cicatrization be complete, a simple pit.
Symptoms of the Confluent Form.—2d. This form has the same initial symptoms as the discrete, but they are of greater severity. The eruption in this variety comes out earlier than in the above-mentioned form. Sydenham early called attention to the fact that the earlier the eruption appeared the more danger there was in its assuming the confluent variety. In this variety the fever does not abate on the appearance of the eruption as it does in the discrete form. The face, hands and feet present an almost continuous pustule, which often bursts in places, and, the pus partly drying, there results a picture which is horrible in the extreme. True pocks nearly always develop in the air passages, and give rise to a copious fetid discharge from the nose and throat. Should the patient recover it is only after a tedious convalescence, with great facial disfigurement and often with defective vision and hearing.
|
|
|
|
|
|
|
Malignant Form.—3d. In some cases this form of the disease is ushered in with a high fever, excruciating pains in the back and vomiting. The hemorrhagic rash appears early, while the hemorrhage takes place from the mucous membrane or surfaces, generally on the evening of the second or third day, and the patient may die in from two to six days, sometimes even before the eruption makes its appearance. The face is swollen and large conjunctival hemorrhages, with the deeply sunken corneae, give a gastly appearance to the features. The mind generally remains clear, but death is the usual result.
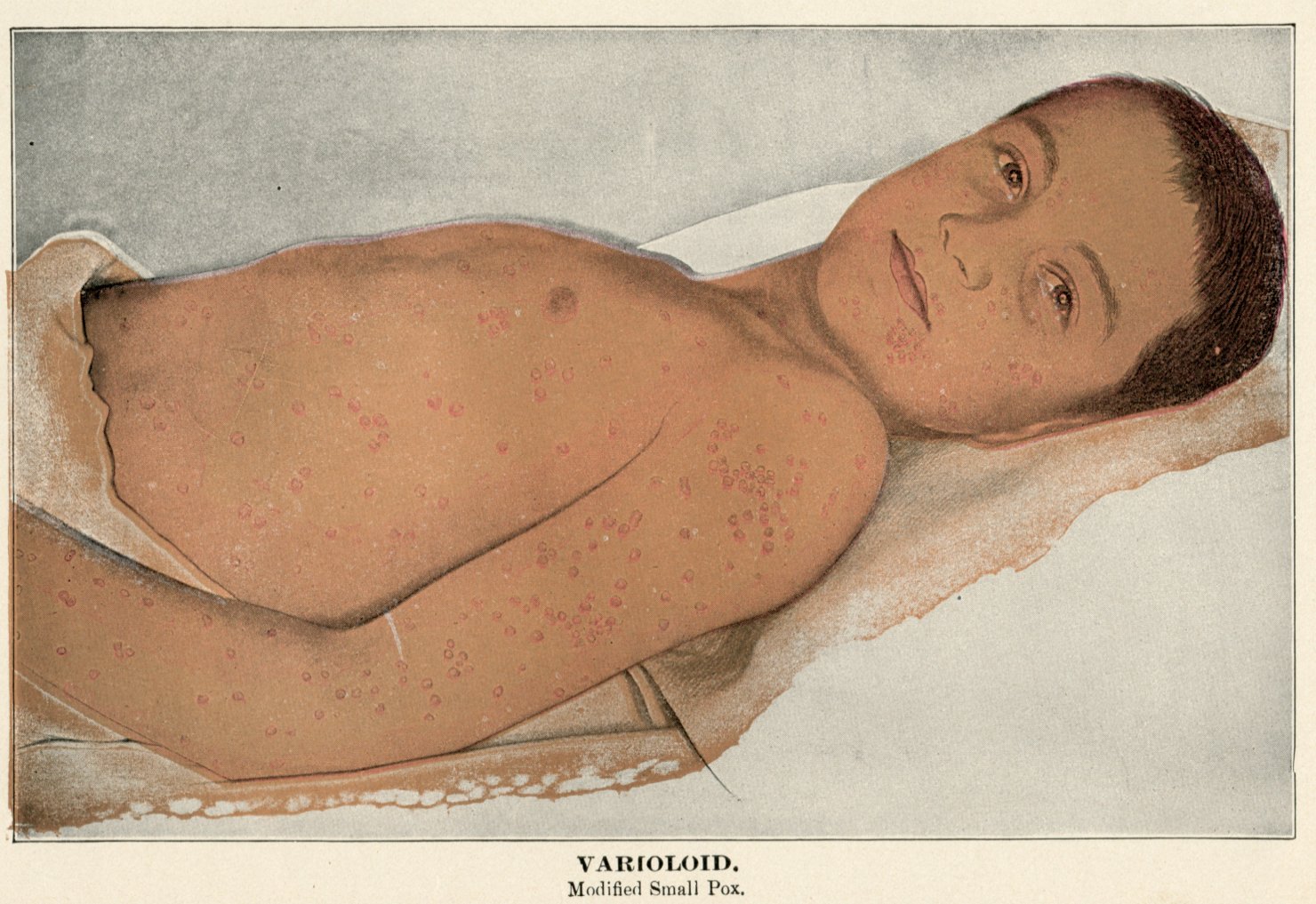
Varioloid.—4th. This is small-pox which is modified by a previous attack, or by vaccination. The attack may come on with the symptoms as severe as in the discrete form, but usually the initial fever is less, the eruption is less general and may abort in its early development, the secondary fever is less marked and convalescence sets in earlier. Vesication, or blistering, takes place rapidly, as there is rarely any scarring.
Diagnosis.—The diagnosis or recognition of small-pox is of great importance, and many an anxious hour is often passed by the physician, the patient, and the friends of the latter before it is possible to decide with certainty as to the nature of the disease. While small-pox may be mistaken for a number of affections, the chief difficulty after the eruption begins to come out is in distinguishing it from measles and from chickenpox. Of course, it is very important to make the diagnosis at the earliest possible moment, in order that timely precautions against the spreading of the disorder shall be instituted. After the pimples begin to contain fluid, the danger of mistaking the malady for measles is over, because the general eruption of measles is never vesicular, although a few little blisters are occasionally seen in bad cases.
To Distinguish from Measles.—In many instances a probable opinion can be given that a disease is measles and not small-pox, from the fact that the eruption of pimples is softer, less shot-like, and arranged in obscurely-defined crescents upon the arms and neck. In others, however, it is impossible to decide before the second day of the eruption, when, as a rule, some few of the pimples will be found slightly vesicular if the disease is small-pox.
|
|
|
|
|
|
|
To Distinguish from Chicken-Pox.—When the vesicles appear, the great point of distinction between them and the vesicles of chicken-pox is that the small-pox vesicle is depressed in the middle, giving it what is called the umbilicated or navel-like aspect. This is an important characteristic, and should always be carefully looked for. Before the eruption comes out, only a probable guess can be made in many instances.
Unusual Symptoms.—Dr. Flint, perhaps the most acute diagnostician in America, says that decided fever following immediately after a chill, the fever continuing without much remission for two days, pain in the back being a prominent symptom, if it be known that the patient has been exposed to small-pox, or if this disease is prevalent, renders the diagnosis extremely probable. In comparatively rare cases, unusual symptoms in an attack of small-pox might for a day or two render the diagnosis difficult from scarlet fever, the simple mild fever called febricula, the skin disease called lichen, some of the pustular eruptions of the venereal disease, and in its very earliest stage from erysipelas and typhoid fever.
Treatment.—Since we have as yet discovered no antidote for the small-pox poison, the chief treatment is the relief of symptoms, as far as possible, as they arise, and careful nursing, in order to avoid needless aggravation of the disease or the development of complications. The mildest cases, as well as those which are more severe, should be kept in bed in a cool apartment, which is ventilated as freely as possible, without producing dangerous draughts.
The Back.—In bad cases the patient's back ought to be frequently examined, and suitable precautions taken against the formation of bedsores, as recommended under the head of typhoid fever, and the hair cut off close, in order to avoid the matting with the corruption from the pustules when that begins to discharge.
The Bowels.—The bowels should be well opened as soon as fever develops with a tablespoonful of castor-oil, or a saline purgative, such as a Seidlitz powder or a bottle of citrate of magnesia, and then a cooling and diaphoretic mixture, composed of half a teaspoonful of sweet spirits of nitre, ten grains of bromide of potassium, and five drops of laudanum, or the one thirty-second of a grain of morphia, administered every two or three hours if there is much pain or restlessness. After the primary fever subsides, with the coming out of the eruption, there are often a few days during which no medical treatment is necessary; but with the appearance of the secondary fever, the cooling mixture should be resumed, or ten grains of Dover's powder may be given at bedtime, and repeated in two hours if the patient is very wakeful or there is much delirium.
|
|
|
|
|
|
|
The Itching.—To relieve the itching, which is sometimes almost intolerable, the surface of the skin may be sponged over with a weak solution of sulphurous acid or of carbolic acid, six or eight drops to the ounce of water. If no relief is obtained from these, anointing the body with cosmoline, or with simple ointment, may be tried; but it is sometimes needful to muffle the hands, especially of children, in order to prevent them from scratching open the pocks after they begin to heal, and so rendering the resulting scars much deeper and more permanent. Keep the patient in a dark room and cover the face with a mask of mercurial or charcoal plaster, so as to shut it from the light; this diminishes the danger of being pockmarked.
The Fever.—The fever, when high, must be kept within limits, either by cold sponging or by the cold bath, the water being at a temperature of 75 degrees when patient is first put in and then gradually lower it to 68 degrees. During convalescence bathing should be frequent, as it helps to soften the crusts. In malignant small-pox, which generally proves fatal, where very soon the face becomes so swollen that the eye-lids are tightly closed and glued together, they should be frequently bathed with a saturated solution of boric acid. The mouth and nose should be kept clean and soft by frequent injections. The patient should have plenty of cold water. Should the heart become weak hypodermics of stychnine, one-thirtieth of a grain, or dram doses of aromatic spirits of ammonia by the mouth.
Treatment of Malignant Small-Pox.—In malignant small-pox, and in the petechial or hemorrhagic form, the black small-pox of common language, the only chance of successful treatment is to support the strength with quinine in four-grain doses thrice daily, or Peruvain bark and other tonics, and with stimulants such as wine or brandy or milk-punch, in the forlorn hope that unusual vigor of the constitution may thus be reinforced long enough for the violence of the disease to become expended. If the patient can thus be kept alive until after the twelfth or fifteenth day without any important organ becoming seriously damaged in its structure, the chance of recovery will subsequently increase every day. The disease being self-limited, it is obviously our chief duty, in the absence of any known specific, to direct all our energies toward sustaining the patient's strength in his battle with the disorder, and the prospect of recovery, or prognosis, as it is termed, turns upon the relative power of endurance of the disease-poison and the patient's constitution.
|
|
|
|
|
|
|
Diet.—The diet in the early stage of small-pox, like that in most febrile conditions, should be light and unstimulating, consisting of rice, cornstarch, bread and milk, or arrow-root. Oranges or lemonade in moderation may be allowed, unless there is a tendency to diarrhoea. Ice water, lumps of ice, or iced carbonic acid water may be given ad libitum. Later on in the disorder, when the strength begins to fail and the pulse grows weaker, strong animal broths, beef essence, and other highly nutritious aliments are necessary; and if the pulse at the wrist should seem very feeble, and especially if it should become intermittent, milk-punch, egg-nogg, or other powerful stimulants ought to be resorted to.
Nursing in Small-Pox.—The general care of a small-pox patient ought to be afforded in accordance with directions contained in the chapter on Nursing, and most of the special precautions for avoiding the extension of the disease, and so forth, have been pointed out in the article on Contagious Influence. On account of the danger of pneumonia and pleurisy, particular watchfulness is needed against taking cold from draughts of air; and during the delirium of the fourth stage, in bad cases, the attendant must be constantly on guard to prevent the patient from injuring himself or others. The nurse should wear an overall and remove it on coming out of the room, and her head should be covered with a cap.
Seeing, then, that small-pox is a most painful, loathsome, and fatal disease, for which we have no cure, it becomes infinitely important to avail ourselves of the protection against its ravages afforded by Dr. Jenner's beneficent discovery of vaccination, a discovery which ought to make his name honorable whilst the world stands.
And yet, strange to say, there are people bearing the general aspect of reasoning beings who oppose vaccination; and in England, where vaccination has been made compulsory by law, a league has been formed to combat its enforcement. Recently the folly of these fanatics met, it is stated, with a most righteous punishment in the following circumstance:
A leading anti-vaccinationist, Escott by name, who refused to have any of his children vaccinated, lately lost two of them and his wife by small-pox. Escott borrowed a suit of clothes from a friend to attend his wife''s funeral, and returned them without disinfection, with the result that the lender caught small-pox and also died of it. Subsequently nearly every house in the neighborhood was infected, producing a local epidemic of small-pox, during which sixteen patients were removed to the pest-house. The only excuse for the obstinacy of such deluded people is, that more than half a century of deliverance from the horrors of small-pox has rendered most persons practically ignorant of its dangers. In the latter half of the eighteenth century, that is, from 1750 to 1800, small-pox attacked almost every inhabitant of England, and about one out of every five seized with it died, whilst nearly another fifth of its victims were disfigured or crippled for life. It is estimated that two-thirds of the blind people in England at that time lost their sight from small-pox. To give an idea of its relative mortality, Dr. Guy states that it caused eighteen per cent of all the deaths, and was one hundred times as fatal as diarrhoea, with its allied intestinal disorders, and six times as fatal as apoplexy, palsy and sudden death taken together.
|
|
|
|
|
|
|
Objections to Vaccination.—These, aside from the mere sentimental ones are that in some instances erysipelas and venereal disease have been apparently caused by it, and that it has been accused of being the means of inoculating the human system with scrofula, consumption and certain cutaneous affections. Now, all of these objections can be removed by the use of what is called bovine virus, obtained direct from the cow, without ever having passed through any human body. Glycerinized lymph is now conceded to be the better vaccine virus.
Duty of Vaccination.—This is rendered far more imperative by the danger which every unprotected person in a community exposes his neighbors to by becoming the starting-point of an epidemic of small-pox. Hence, although a man may have the privilege of thus trifling with his own life and health, he has no right to imperil others by his perversity or ignorance; and the good of society, which is a higher law than that of personal liberty, demands that compulsory vaccination be legally established, as it is hoped it will be ere many years elapse.
Making Sure of Immunity.—Even after exposure the individual should be vaccinated, for though it may not prevent small-pox, if will certainly moderate the severity of the attack. The writer has had a case of this kind to come under his personal observation.
How Produced.—This disease, called Vaccina in medical books, is induced in the human being by the process of vaccination, either accidentally, as in the case of the young milkmaid who led Dr. Jenner to his grand discovery, or, as is usual nowadays, by being rubbed into a slight wound made for the purpose. It is apparently a modified form of small-pox, in which a cow-pox vesicle on the udder of a cow or heifer is the common original source of the infecting matter.
|
|
|
|
|
|
|
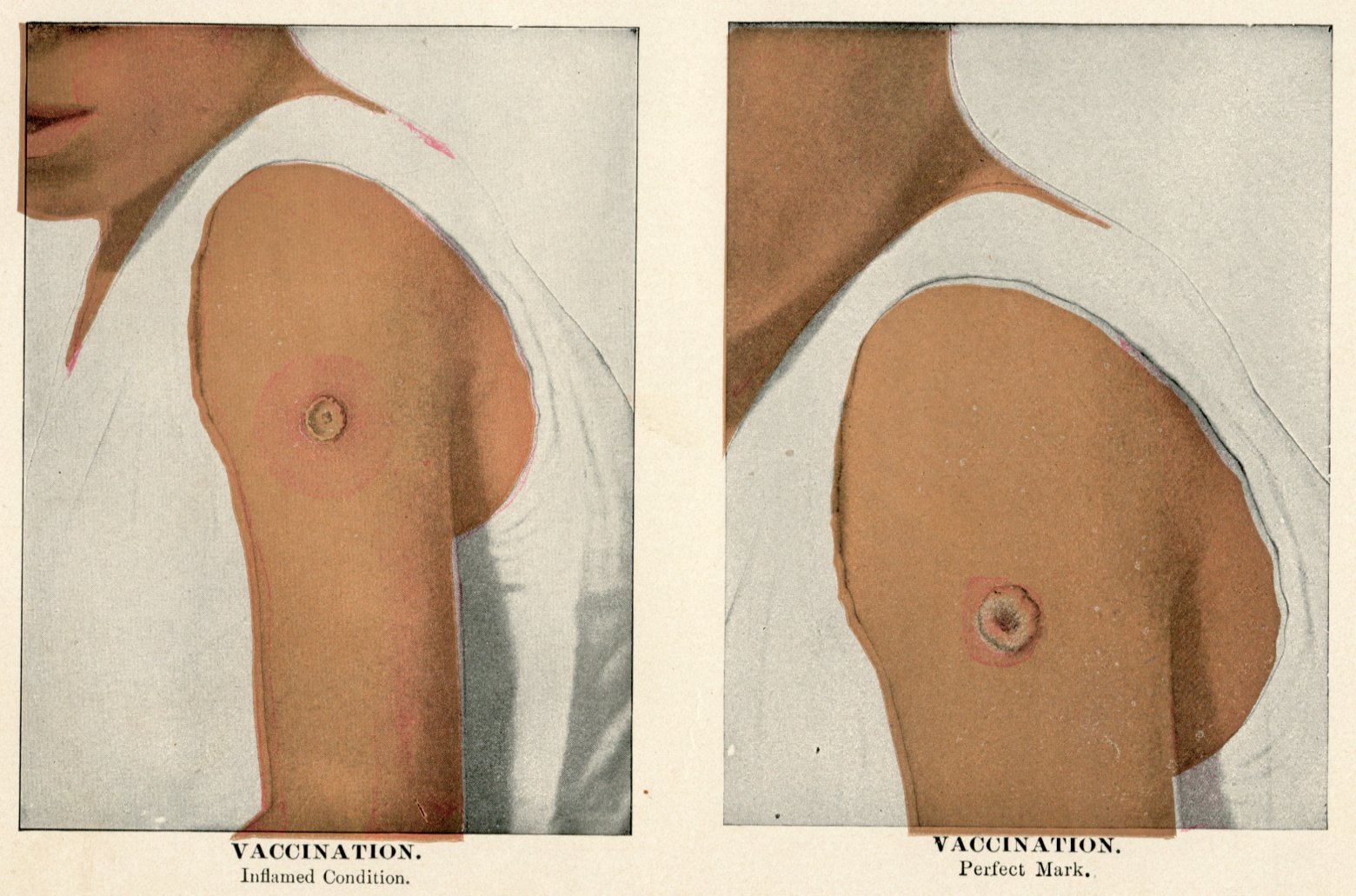
Character.—The disease is attended, as a rule, with no further eruption than the vesicle, ripening into a pustule at the point or points where the matter is inoculated. It is communicable by inoculation, but not by the other ordinary modes of infection, mild in its course, and yet, generally speaking, protective against small-pox,
Operation of Vaccination.—This is by no means so simple and unimportant as it seems at first sight, and it therefore ought always to be performed by a physician. It is better not to cut so deep in vaccinating as to cause much of a flow of blood, lest this fluid should wash the virus out of the incisions. The usual place for vaccinating is on the outside of the arm, an inch or two below the shoulder; but if the operation fails here, as is sometimes the case after repeated trials, an attempt may be made on the calf of the leg, just below the knee.
When to Vaccinate.—Vaccination should be performed on all children between the ages of one and three months, unless some special reason exists for its postponement, and it is recommended to insert the virus in four or five places close together, so as to produce several pustules, although, by a majority of physicians in this country, one pock is thought sufficient.
Revaccination.—Revaccination should be performed about once in seven years, as in some instances the protection afforded appears to wear out in that time; and, as there is no means of recognizing them, the safer way is to renew the vaccination.
The Virus.—The animal or bovine virus is supplied from carefully vaccinated calves by a number of producers in various parts of the country. It is usually furnished on little ivory points, shaped like a lancet-blade, or on pieces of quills. Either of these is to be moistened, in pure water, and then rubbed on a lightly scarified surface, prepared as already described. The bovine virus is apt to make a very sore arm, but has the great advantage of avoiding all possibility of introducing the horrible poison of venereal disease into the blood of the infant operated upon.
For full description and treatment of this disease, peculiar to children, see CHILDREN'S DISEASES, Book IV, Part XII.
|
|
|
|
|
|
|
For full description and treatment of measles, see Book IV, Part XII, DISEASES of CHILDREN.
Definition.—An acute infectious disease resembling both scarlet fever and measles, but differing from these in its short course, slight fever and freedom from complications.
Cause.—It is propagated by contagion and spreads with great rapidity.
Incubation.—About two weeks.
Symptoms.—This is a mild contagious affection, very similar in many respects to ordinary measles, but apparently differing from it, because neither disease affords any protection from the other. The color of the eruption is rather more a rose-tint than in ordinary measles, the pimples are round instead of oval, and the crescentic arrangement is wanting or extremely obscure. Children are chiefly affected with German measles, although it also occurs after adult age is attained, but in any case the malady is so slight that the patients rarely feel sick enough to keep in bed, and no instances of death from the uncomplicated affection are recorded.
Treatment.—The treatment, diet and nursing appropriate to German measles are the same as those recommended in the ordinary form, in the few cases where any special care is needed.
For description and treatment of scarlet fever, see DISEASES of CHILDREN, Book IV, Part XII.
Synonyms.—Dandy, or break-bone fever.
Definition.—An acute and infectious disease characterized by febrile paroxysms; pain in the muscles and joints and sometimes by an eruption on the skin.
History and Geographical Distribution.—The disease was first recognized in 1779 in Cairo and in Java. The description by Benjamin Rush of the epidemic in Philadelphia in 1780, is one of the first and one of the very best articles ever written on the disease. S. H. Dickson gives a graphic description of the disease as it appeared in Charleston in 1828. Since that date there have been five or six widespread epidemics in tropical countries, the last occurring along the Gulf States in the summer of 1897, where for some time it was supposed to be yellow fever. None of the recent epidemics have extended to the Northern States, but in 1888 it prevailed as far north as Virginia.
|
|
|
|
|
|
|
Cause.—The rapidity of diffusion and the pandemic character are the two most important features of dengue. There is no disease, not even influenza, which attacks so large a proportion of the population. A micrococcus has been found in the blood of patients by McLaughlin, of Texas.
Symptoms.—Incubation—Three to five days, during which the patient feels well. Persons who catch this curious complaint are often attacked with it very suddenly, frequently in the night after retiring in their usual health. The temperature rises in a few hours to 103 degrees and in one or two days may reach 106 or 107 degrees, the skin becomes dry and hot, and the countenance indicates utter helplessness and prostration; with this febrile condition, there is usually pain in the head, back, limbs and small joints, which latter swell up as in rheumatism. The pulse is rapid; loss of appetite, coated tongue, slight nocturnal delirium and concentrated urine. The pain may be so severe that the patient cannot move.
Duration.—The average duration of the first febrile stage is about forty-eight hours, although it may vary from twelve hours to three days, after which the symptoms begin to subside and a period of remission of two or three days occurs.
Debility and Eruption.—During this time general debility and muscular pains predominate, and fever is usually absent, but on the fourth day it reappears, and on the fifth or sixth an exanthematous eruption develops, which is sometimes more like the flush of erysipelas than the papules of either measles or scarlet fever. The color, however, is not so intense, and it spreads over the whole body in forty-eight hours.
Pains and Swelling.—When the eruption reaches its height, painful swellings of the lymphatic glands of the neck, back of the head, armpits and groins occur. With this tumefaction of the glands, the nose, mouth and throat become implicated, swelling up and growing excessively painful. On the seventh or eighth day desquamation commences and the acute stage terminates.
Malady Not Fatal.—The victims of dengue are to be commiserated for the horrible and agonizing pains which they are called upon to suffer, and which are peculiar to the disease; but they may find some comfort in the assurance that the malady is rarely, if ever, fatal.
|
|
|
|
|
|
|
Recurrence of Pain.—The recurrence of the excruciating pains in the limbs at a time long after the subsidence of the fever must be borne in mind, as influencing any opinion ventured in regard to the probable duration of the illness.
Diagnosis.—The diagnosis of dengue must occasionally be made from rheumatism, measles, scarlet fever and erysipelas; but a complete history of the case can hardly fail to clear up any doubts, particularly if dandy fever is prevailing in the locality as an epidemic.
Remedies.—Since the malady is not a dangerous one, anodynes to relieve the excruciating suffering, especially hypodermic injections of one-eighth or one-sixth of a grain of morphia. During convalescence iodide of potash is recommended for the arthritic pains and tonics are indicated.
Synonyms.—Ship, jail or putrid fever.
Definition.—An acute infectious disease favored by closely crowding human beings together, characterized by sudden onset, a maculated rash, marked nervous symptoms and a termination by crisis about the end of the second week.
Causes.—It is excited by an unknown poison which is capable of being carried in the clothes. It is rare in America, though there were two mild epidemics in the Philadelphia Hospital in 1866 and in 1883; it is not uncommon in England and Ireland. Bad food, impure air and overcrowding are predisposing factors.
Incubation.—Incubation is placed at about twelve days, but may be less., and its duration from ten days to two weeks.
Symptoms.—The fever begins abruptly with severe pain in the head, back and limbs; extreme prostration, and fever which reaches its maximum (104 degrees to 105 degrees) in two or three days. The temperature remains high for about ten days when it falls by crisis (suddenly).
The Eruption.—It is a continued fever, attended with a dark-red or purplish mottled rash over the body, with great nervous prostration, restlessness and delirium, or dullness and stupor, but without any specific affection of the bowels. The eruption, which makes its appearance from the third to the eighth day of the disease, is at first slightly elevated and disappears when pressed upon with the finger; but after the second day from the time it comes out, it is persistent under pressure and continues to show this character until it fades ten or twelve days afterward.
Fatality.—When it proves fatal, as it does in about fifteen per cent. of the cases, death usually occurs between the twelfth and twentieth days of the attack.
|
|
|
|
|
|
|
Advent Symptoms.—The advent of the disease is somewhat gradual, beginning with general soreness, discomfort and weariness, with loss of appetite and disturbed sleep. Shivering and a feeling of coldness, especially along the spine, sometimes amounting to an actual chill, not unfrequently mark the commencement and are soon followed by heat of skin, rise in temperature and severe frontal headache. This headache is occasionally very severe and rarely absent at first, but abates about the tenth day.
Disturbed Sleep.—Slumber is disturbed by dreams, is unrefreshing, and when the patient is not asleep there is a constant tendency to heaviness, the mind ceases to think and the attention cannot be concentrated upon any subject. He may lie with his eyes open, evidently not in slumber, yet indifferent or insensible to all which goes on around him.
Bodily Weakness.—This is frequently extreme, and the sufferer often voluntarily takes to his bed on the first day of his illness. This exhaustion and prostration is totally disproportionate to the amount of muscular exertion which has been made. The eyes, when examined, are found to be dull and heavy, the white portion injected or blood-shot and a peculiar dusky flush overspreads the cheek.
The Delirium.—As the days pass debility rapidly increases and delirium comes on the latter part of the first or early in the second week. In persons of nervous, excitable temperament it commences sooner and may appear on the third or fourth night of the fever, showing itself primarily, perhaps, by a little confusion of thought on awaking from a restless doze.
The Tongue.—The tongue is coated at first with a white fur, but after six or eight days often may become dry, swollen and covered with thick, brownish crusts of mucus and cast-off epithelial cells, which make up what is called sordes.
The Bowels.—The bowels are, as a rule, constipated, and this should especially be borne in mind, because it forms an important distinguishing mark between this disease and typhoid fever, with which typhus was formerly confounded.
The Pulse.—The pulse is quickened from the outset and in grave cases continues to increase in rapidity until it may more than double its ordinary frequency, beating from one hundred and forty to one hundred and sixty times per minute.
Complications.—Brocho pneumonia is perhaps the most common complication. It may pass on to gangrene; in certain epidemics gangrene of the nose, hands and toes have occurred.
|
|
|
|
|
|
|
Diagnosis.—The diagnosis of typhus fever requires to be made in this country chiefly from typhoid fever and relapsing fever, but it is sometimes difficult to distinguish it at first from small-pox, plague, erysipelas and cerebro-spinal meningitis.
Treatment.—As the treatment, diet and nursing of typhus fever are similar in most respects to what is required in the far more common disease, typhoid fever, the reader is referred to our article upon the latter affection for further information.
Isolation.—When an epidemic of typhus fever breaks out in a crowded jail, hospital or tenement, the great cause of its prevalence should, of course, at once be abolished, by separating those exposed to it as widely as possible and treating the sick in isolated sheds, huts or even in tents.
Synonyms.—Enteric fever, autumnal fever or typhus albuminalis.
Definition.—An acute infectious disease due to the implantation and proliferation of the bacillus of Eberth, characterized by ulceration of the lymph follicles of the intestines of the mesenteric glands and by an enlargement of the spleen.
Historical.—The disease is easy recognizable in the descriptions of Hippocrates (B. C. 460-357) and Galen (A. D. 130-200). Doubtless John Huxam's "slow, nervous fever," described in his "Essay on Fevers" was the typhoid of the present day, and his "putrid malignant" the yellow fever of to-day. It was, however, the writings and teachings of the great French physician, Louis, which did most to disseminate a knowledge of the true nature of typhoid fever, to which he gave the name it bears. Among some of his pupils were the Americans W. W. Gerhard and C. W. Pennock of Philadelphia and James Jackson, Jr., of Boston. To the former, however, is due the great honor of having first clearly laid down the difference between typhoid and typhus.
Causes.—Typhoid fever prevails in temperate climates in which it constitutes the most continued fever. It is widely distributed throughout all parts of the world.
Seasons.—It prevails most in the autumn months, especially following a dry summer.
Sex.—Males and females are equally liable.
Age.—Typhoid fever is a disease of youth and adult life. The greatest susceptibility is between the ages of fifteen and twenty-five. It is rare after sixty and infants are seldom attacked.
|
|
|
|
|
|
|
Immunity.—As in other fevers, not all exposed to the infection take the disease. Some writers claim that one attack protects, but others claim that one attack predisposes to another.
Bacilli in the Body.—The bacilli are found in the lymphoid tissues of the intestines, in the mesenterie glands, in the spleen, liver, bile and in the bone marrow. They also occur in irregular clumps in the contents of intestines and in the stools; they have also been found in the blood, urine, sweat and sputa.
Bacilli Outside the Body.—The bacilli retain their vitality in water for weeks, but disappear from ordinary water in competition with saprophytes in a few days. In milk they undergo rapid development without changing its appearance. They may increase in the soil and retain their vitality for months. They are not killed by freezing, but, as Pruden has shown, may live in ice for months.
1. Contagion.—The possibility of the direct transmission through the air from one person to another must be acknowledged, although, as shown by Germano, when completely dried in air currents, the specific bacillus quickly dies. There are house epidemics in which water and food contamination can almost be excluded. The nurses and attendants who have to do with the stools and body linen of the patient are alone liable to direct infection.
2. Infection of Water.—This is unquestionably the most common mode of conveyance. Many epidemics have been shown to have originated in the contamination of a well or a spring.
3. Milk.—Milk may be the source of infection, as it may be contaminated in washing out the cans with infected water.
4. Ice and Salads.—In addition, the germs may be conveyed in ice, salad, celery, and so forth. A fly which has alighted on the soiled linen of a patient may contaminate the milk or food.
Bad Sewage and Drainage.—Filth, bad sewers or cess-pools cannot in themselves cause typhoid fever, but they furnish the conditions suitable for the preservation of the bacillus.
|
|
|
|
|
|
|
Symptoms.—Typhoid fever, also called gastro-enteric fever, owing to the circumstance that the stomach and intestines are the chief seats of the disease, is characterized by a faint, scanty eruption of rose-colored spots, appearing chiefly upon the abdomen, from the fourth to the eighth day, and coming out in successive crops. Each crop of spots continues visible for about three days.
Cess-Pool Fever.—On account of its frequent connection with bad drainage, this fever has received the vulgar but expressive name of "drain or cess-pool fever," which, despite its indelicacy, it would be well to perpetuate as a constant warning against that neglect of sanitary arrangements in buildings to which it is chiefly due.
Initial Symptoms.—The onset of this dangerous and fearfully prevalent disease is very often a gradual one. The patient for some days feels weak, languid and depressed, loses his appetite, suffers from headache, and is restless at night. In other cases, however, the malady begins with a slight chill, or a feeling of coldness running up and down the back, and among children the first decided symptom may be an attack of convulsions. Frequently, too, slight bleeding of the nose is noticed, and a little tendency to looseness of the bowels, which may even be aggravated by errors in diet, or other imprudence, into active diarrhoea.
Secondary Symptoms.—After the stage of invasion is completed, the pulse and temperature rise steadily, the former going up to 100 degrees or 110 degrees, and the latter ascending to 104 degrees, or sometimes 105 degrees during the first week. The heat of the body is almost always greater at night than in the morning, and this increment is so regularly advanced during the onset of the disease, that it is quite possible for a skilled physician to recognize typhoid fever by a glance at the record of temperature, or "temperature chart," alone in many instances.
The Diarrhoea.—The diarrhoea rapidly grows more severe, and in bad cases is frequently very profuse, fifteen or twenty thin, watery evacuations occurring in every twenty-four hours. Pain in the abdomen, especially in the region of the right flank, is nearly always complained of, and with the diarrhoea is due to the characteristic ulceration of certain oval spots in the lower portion of the small intestine, which have received the names of Peyer's patches. Bronchial irritation and cough are common.
Facial Appearance.—The face sometimes wears an anxious, haggard look, but frequently, even early in the disease, it shows the dull, indifferent aspect, so often indicating an oppression of the brain, which will deepen into stupor, then coma and finally death. The flush of the face is apt to have a more dusky, purplish tint than in other fevers, and the skin is more dry and burning, or pungent, from the smaller amount of perspiration.
|
|
|
|
|
|
|
The Delirium.—In the second week delirium generally comes on, and although occasionally violent and requiring the patient to be controlled by physical force, it is more frequently of a low, muttering character. The tongue becomes dry and brown, and tympanites, or the accumulation of gas in the bowels, is generally considerable, and may cause by its enormous distension great suffering, or even lead directly to a fatal result. Ringing or buzzing in the ears with deafness is very often noticed. In bad cases the diarrhoea is often very profuse, and discharges of fluid blood, perhaps in large quantity, sometimes occur and prove quickly fatal.
The Third Week.—In the third week, if the case is to end unfavorably, the pulse grows frequent and feeble, the tongue is dry, cracked and covered with brown sordes, the delirium and stupor are constant, involuntary discharges from the bowels occur, and the patient may die exhausted, or if the fatal issue comes earlier, before complete prostration of muscular strength, it may be preceded by convulsions.
Signs of Recovery.—If, on the contrary, recovery awaits the patient, the pulse falls off in frequency, the temperature gradually diminishes, the tongue cleans off usually from the edges, appetite slowly returns and the mental powers are little by little regained.
Unfavorable Symptoms.—The unfavorable symptoms, besides those above mentioned, are an unusually high temperature, 106 degrees or over, picking at the bedclothes, slipping down in the bed, and entreaties, often of pitiful earnestness, to be taken home.
Special Features and Symptoms.—1. A severe facial neuralgia may put the practitioner off his guard. In cases when the patient has kept up, "fought the disease," the first manifestation may be a pronounced delirium. In rare cases the disease sets in with the most intense cerebro-spinal symptoms, simulating meningitis.
2. There may be pronounced pulmonary symptoms. In a few cases the disease sets in with a single chill, with pain in the side and all the characteristic features of lobar pneumonia.
3. There may be intense gastro-intestinal irritation. Occasionally there are cases with such intense vomiting and diarrhoea that poisoning may be suspected.
Fever.—The fever has invariably a step-ladder rise; the evening temperature is from one to one and one-half degrees higher than the morning remission.
Fever of Convalescence.—After the temperature has been normal for five or six days the fever may rise suddenly to 102 degrees or 103 degrees, and after persisting from one to three or more days fall to normal. With this condition there is no furring of the tongue and no distention of the abdomen. This condition is by no means uncommon, and is of especial importance, as it is attributed in most cases to errors in diet, constipation, or excitement of any sort, such as seeing friends.
|
|
|
|
|
|
|
Complications.—1. Thrombosis of the femoral vein, more frequently on the left side, resulting in the "milk leg." It occurs, according to Murchison, in one per cent. of all cases. Embolic abscesses may occur in the kidney and lungs.
2. Albuminuria is present to some extent in all severe cases, commonly as the result of the fever, but sometimes is the direct result of an acute nephritis.
3. Hemorrhages usually occur during the third week, and are indicated by a sudden fall of temperature, followed by dark red or tarry stools.
4. Cardiac complications, including pericarditis, endocarditis and myocarditis, are sometimes present. The latter may be the cause of sudden death.
5. Typhoid fever predisposes the patient to tuberculosis.
6. Peritonitis may result from perforation or from extension by continuity; the former is more common and is recognized by a sudden pain, a fall of temperature, distention of the belly and symptoms of peritonitis.
7. Pneumonia may supervene in the second or third week of a typhoid fever, as a complication, in which the true relation is difficult to determine.
Diagnosis.—The diagnosis of typhoid fever must be made in its early stage from typhus fever, relapsing fever, scarlet fever, measles and small-pox. At a more advanced period it might be confounded with the typhoid condition met with in uremia and pyemia, and also with enteritis or inflammation of the bowels, peritonitis or inflammation of the membrane covering the intestines, meningitis or inflammation of the membranes of the brain, acute bronchitis or pneumonia, and with acute consumption.
The Rose-Colored Spots.—If a patient who has been suffering from headache, prostration, loss of appetite, restlessness and gradually increasing fever, has a slight bleeding at the nose unprovoked by accident, we may strongly suspect typhoid; but until the rose-colored spots appear there is no certainty.
Treatment.—The medical treatment in typhoid fever must be directed toward mitigating suffering, warding off complications and obviating the tendency to death. In the early stages of the complaint headache is one of the most prominent symptoms. All we can hope for is to procure some mitigation of the intense suffering it frequently occasions.
|
|
|
|
|
|
|
Ice Application.—The application of ice to the head, either in a bladder or India-rubber bag, or, what is still better, by means of an ice-cap, made of numerous coils of thin rubber pipe, through which ice-water is kept flowing, generally diminishes the pain, which, if very intense, may require the application of one or two leeches behind the ears.
For Checking Diarrhoea.—Diarrhoea, if troublesome, is to be checked, but not stopped, by chalk-mixture, bismuth-mixture or astringents with opium, as
Morphine sulphate ............................ 1 grain
Creosote ..................................... 6 drops
Bismuth subnitrate ........................... 3 drachms
Mix and make into 12 papers and take one every three hours.
Or, when ordinary measures fail—
Silver nitrate ............................... 6 grains
Extract of opium.............................. 4 "
Mix and put into pills, making 20. Take one every three hours.
Its use, however, after the first few days, must be continued with great caution, on account of permanently blackening the patient's skin.
Rest.—Absolute rest in bed, with the use of the bed pan, must be enforced.
Rendering Stools Innocuous.—The stools should be rendered innocuous. This may be done by dissolving a pound of the chloride of lime in four gallons of water. Add a quart of this solution to each discharge and allow it to remain in the vessel at least an hour before disposing of it. Soiled bed clothes should be thoroughly boiled.
Restlessness.—In cases where restlessness rather than stupor predominates, ten grains of Dover's powder, or a draught composed of twenty drops of laudanum and ten of antimonial wine, will frequently moderate the excitement in a very favorable manner. When the tongue becomes dry, ten drops of the oil of turpentine given in mucilage every four hours, often have a very happy effect, and its influence upon the healing of the intestinal ulcerations is highly lauded.
Stimulants.—Generally, during the second week, sometimes a few days earlier, and occasionally a few days later, according to the violence of the attack and the patient's strength of constitution, it is advisable to begin with the use of stimulants. The best indication of their becoming needful is a slight failure of the strength of the pulse, but much experience is necessary to judge correctly of the time, the quantity, and the frequency with which alcohol should be administered.
|
|
|
|
|
|
|
Kinds of Stimulants.—At first half an ounce of good whiskey or brandy, with two or three ounces of milk and half an ounce of lime-water, if nausea persists, may be allowed three times daily, but this amount must generally be increased from day to day, sometimes with great rapidity, until in the worst cases a pint and a half of brandy is swallowed in twenty-four hours. Beef-tea, beef-essence, and some farinaceous food, such as arrow-root or cornstarch, ought also to be urged upon the patient at this time.
To Stop Hemorrhages.—In cases of hemorrhage from the bowels, ten grains of kino, a teaspoonful of syrup of rhatany, or ergotin hypodermically, in full doses, afford the best chance of success; and if perforation of the intestine, in consequence of the eating through of one of the ulcers, takes place, the very slender hope of recovery is increased a little by the administration of large doses of a grain every hour of opium and by securing perfect rest in bed.
Hydrotherapy.—Since many of the worst symptoms of typhoid fever seem to be due to the effect of overheated blood upon the brain, efforts to reduce the temperature by the aid of cool baths of about 70 degrees Fahrenheit six or eight times daily, or cold sponging of the whole body, have of late years taken a very prominent place in the treatment of the disease, and are believed to reduce markedly its rate of mortality. Where, in spite of judicious employment of means to bring down the temperature, unconsciousness continues, great watchfulness is necessary in regard to the evacuation of the bladder, which may become dangerously distended, and even burst for want of attention.
Drawing the Urine.—When examined and found to be over-full, the urine should be at once drawn off by means of a catheter, and the operation repeated twice or thrice every twenty-four hours, until the patient resumes control over his functions.
Other treatment would be the
1. Sponge Bath.—The water should be cold or ice-cold, according to height of fever, and a thorough sponge bath should take from fifteen to twenty minutes. I have added alcohol to the water with good results.
2. Cold Pack.—If tub is not available the patient may be wrapped up in a sheet wrung out of water at 60 degrees to 65 degrees and then cold water sprinkled over him with a watering pot.
|
|
|
|
|
|
|
3. The Bath.—The tub should be long enough so that the patient can be completely covered, except his head. Every third hour, if temperature is above 102 degrees, the patient is placed in a bath at 70 degrees Fahrenheit, which, after the patient is put in, can be lowered a degree or two. In it he remains for fifteen or twenty minutes. He is then taken out, wrapped up in a dry sheet and covered with a blanket. The patient's limbs and body are gently rubbed while in the bath, and on removing he should have a stimulant. Rectal temperature should be taken directly after the bath, and again forty-five minutes later. Should the patient be too weak for the bath, frequent sponging or Leiter's coils should be used.
Constipation.—Should constipation be present, though as a rule it does no harm, it is well every third or fourth day to give an enema. If a laxative is needed during the disease give Hunyadi-Janos water.
Hemorrhage.—Should hemorrhage exist it should be treated with full doses of opium and acetate of lead. Ice should be freely given, and food should be restricted for eight or ten hours. If there should be any symptoms of collapse give stimulants.
Diet.—The diet of a typhoid fever patient must be watched over with unceasing vigilance, as upon it and proper nursing, more than upon medical treatment, the chances of success often depend. In the first stages it should be light, entirely unstimulating and unrelaxing to the bowels.
No Solid Food.—Throughout the whole course of the disease no solid food ought to be allowed, and this precaution should be rigidly enforced on account of thereby avoiding the risk of mechanically rupturing some little hole in the intestine, at the seat of an ulcer which had almost perforated the wall of the bowel. Such a catastrophe must, as already hinted, lead to almost certain death.
Drink.—As the thirst is usually very great, whilst the appetite is nearly lost, it is a good plan to make the drinks somewhat nourishing in order to support the strength. Hence, gum-arabic water, barley-water, or milk thickened with tapioca, sago or cornstarch are often highly advantageous.
No Fruits.—If the usual tendency to diarrhoea is at all marked, fruits of all kinds ought to be entirely withheld by the nurse, and even where the bowels are not disordered, fruits and vegetables, other than those enumerated, should be very cautiously given, on account of the disposition to looseness of the bowels which generally exists. Many cases of death from typhoid fever may be directly traced to the murderous imprudence of nurses and attendants in this respect.
|
|
|
|
|
|
|
Diet for Second Week.—During the second week, when slight indications of debility usually begin to manifest themselves, a more nutritious diet becomes necessary. Thicker preparations of the farinaceous, foods above mentioned should be employed, beef-tea and beef-essence may be added to the list, and as debility increases eggs beaten up with milk; flavored perhaps with a little wine, if they have been well borne during health, may be administered. In the latter stages, when the whole capacity of the enfeebled digestive organs is needed to take up sufficient food to sustain life, strong meat-soup, beef-essence, eggs beaten up with wine, and milk punch should alone be urged upon the patient.
Injected Food.—Life has apparently been saved in some instances by frequently repeated small injections of beef-essence, brandy and milk, with a few drops of laudanum, in order to prevent the enema from being rejected from the bowels, as is too often the case in spite of all our efforts.
Nursing.—In nursing the case of a typhoid fever patient, watchful and judicious care of a skillful attendant often contributes in those instances having a favorable termination, as most candid physicians will admit, more than medical treatment to the sick man's recovery. The suitable administration of medicines to control diarrhoea, acording to the varying phases of that important symptom; to relieve restlessness and allay excitement; the proper employment of baths to reduce febrile heat and diminish cerebral congestion; the constant guarding of the patient from injurious articles of food; the increasing effort to economize the failing strength, which otherwise may prove just a little lacking in the last great day of struggle with the disease, notwithstanding all the reinforcements called upon in the way of stimulants and nutrients to support it, all these offer an ample field for the highest intelligence and the noblest self-sacrifice.
Watching the Delirium.—The attendant upon a typhoid fever case must be on his guard, lest in his momentary absence the delirious patient gets out of bed and attempts to escape from the house, or perhaps throws himself out of a window. Even the effort at walking across the room may, in the weak conditions met with in the latter portion of the fever, so exhaust the failing strength as to lead to dangerous or fatal collapse.
Treating Bed-Sores.—The tendency to bed-sores, which are particularly apt to form over the portions of the body pressed upon in lying upon the back during typhoid and typhus fevers, must be overcome, as far as possible, by frequent change of position, the use of perforated pillows or cushions and of water-beds, and the patient should be well rubbed with alcohol twice a day, especial care being used over the parts of the body that the patient rests on while in bed, i. e; back, buttock, and so forth. As a general rule, the formation of a bed-sore in a case of typhoid fever not lasting more than twenty-five to thirty days, is evidence of carelessness on the part of the nurse, and should never be permitted to occur. When once developed, bed-sores must be kept clean and carefully dressed once or twice daily, in the hope of preventing them from spreading, as the chance of curing them until the patient can sit up is exceedingly small. Not only is the suffering from bed-sores very great, but the free discharge of pus which they generally yield is extremely debilitating and quickly exhausts the little remaining stock of strength.
|
|
|
|
|
|
|
Typhoid Mortality.—The mortality of typhoid fever varies in different epidemics from 10 to 20 per cent. The older the patient the less is his chance of recovery from the malady, whilst among children the proportion of deaths is quite small.
Walking Typhoid.—Some of the mildest cases, those to which the name of "walking typhoid" has been appropriately applied, may suddenly terminate in perforation of the bowel, and death in a few hours from collapse or from peritonitis. On this account a typhoid fever patient, no matter how slight his symptoms of illness may be, should stay in bed, and swallow nothing but liquid food, until the searching test of the thermometer shows that all febrile movement has subsided.
Management of Convalesence.—Even after convalescence has fairly set in, great watchfulness is necessary. Permission to sit up in bed even ought not to be given until several days have passed without any fever, as proved by the thermometer, which should be used morning and evening throughout the complaint, and the return to solid food must be both slow and gradual. Any imprudence in diet, or slight over-exertion, may bring on a relapse, which is much worse than the original attack, and its causes ought therefore to be most seduously shunned.
Prevention of Typhoid.—The great means of preventing typhoid fever by unceasing vigilance in regard to the purity of the water-, milk- and air-supply has already been urgently insisted on.
Definition.—An infectious disease occurring sporadically and in epidemics, caused by a diplococcus, characterized by an inflammation of the cerebro-spinal meninges and symptoms of great pain in the head, back and limbs, convulsions, irregular fever, and at times petechial eruption.
History.—In 1801 Vieussens first described a small outbreak in Geneva. There had been several outbreaks in the United States prior to 1875, but since that time there have been several extensive epidemics. There was a serious epidemic in Western Maryland in 1893, in New York in 1893, and from the spring of 1896 to the spring of 1898 the disease has prevailed extensively in Boston and its neighboring towns.
|
|
|
|
|
|
|
Causes.—Over-crowding, poor food, foul air and bad drinking water seem to be the predisposing causes. The epidemics have occurred most frequently in winter and spring. The concentration of individuals, as of troops in barracks, seems to be a special factor; in civil life children and young adults seem most susceptible.
Symptoms.—Many different forms have been described, but they are best grouped into three classes:
1. Ordinary Form.—This is a malignant epidemic fever, usually attended with painful contraction of the muscles of the neck and retraction of the head, and frequently accompanied by a profuse purpuric eruption, It is a disease which generally comes on suddenly, runs its course with great rapidity, and proves fatal in a majority of instances. The malady is more than a mere inflammation of the membranes of the brain, or meningitis, for the whole nervous system seems to be very gravely affected from the first.
Premonitory Symptoms.—Premonitory symptoms are rare, but when they are met with, show themselves simply as slight headache and pain in the back, or a little uneasiness and weariness experienced for several days before acute symptoms set in. These may commence with a chill or marked shivering-fit, followed by intense vertigo, headache of intolerable severity, obstinate and violent vomiting, painful muscular stiffness, soon developing into continuous spasms, affecting particularly the muscles of the head and back.
Head Distress.—Distress in the head is constant so long as consciousness lasts. The eyes are blood-shot, and express agonizing suffering, the pupils are contracted, and the countenance is pale. Excessive restlessness and general muscular agitation prevail, and the sensibility of the whole surface is so great that every touch and movement causes excruciating pain, and even touching the hair is painful.
Third Day Symptoms.—These symptoms increase up to the third or fourth day, when the power of swallowing begins to be affected, and the process of respiration to be imperfectly and irregularly performed, the head being dragged tightly back as far as possible, and the features fixed in the horrible and characteristic grin of lockjaw. The delirium usually developed during the third day, if it has not sooner appeared, passes into stupor, and this in its turn deepens into coma, from which or from suffocation death commonly releases the sufferer between the fifth and eighth day of the complaint, or in a few cases the patient may gradually improve, and after three or four weeks enter upon a tedious convalesence of many months' duration.
|
|
|
|
|
|
|
2. Malignant Form.—There is an abrupt onset with a chill, followed by vomiting, headache, moderate fever, convulsions and rash.
3. Abortive Form.—The disease begins abruptly with grave symptoms, but terminates in a few days in recovery.
Diagnosis.—The diagnosis between this disease—which, it should be stated, has also been named epidemic cerebro-spinal meningitis, or purpuric fever—and typhus fever, typhoid fever, tetanus or lockjaw, tubercular meningitis and typhoid pneumonia, is usually not difficult, except in the earliest stages. The fact of its epidemic prevalence generally aids at once to its recognition, except in the first few cases which occur, and even in these the intolerable headache, retraction of the head, and excessive sensitiveness of even the hair to the lightest touch, are almost always sufficient to characterize this strange and terrible malady.
Complications.—Deceptive vision from inflammation of the cornea or atrophy of the optic nerve; defective hearing from inflammation of the auditory nerve or from suppurative inflammation of the middle ear. Pleurisy, pericariditis and parotitis are not uncommon and headaches more or less severe may remain for months or years.
Treatment.—The treatment consists of dry or cut cups to the nape of the neck and along the spine, cold to the head by means of ice-bags or bladders, or better still the ice-cap, opium in quantities of a grain every two or three hours, and especially hypodermic injections of morphia, to relieve the agonizing suffering as well as for the direct curative effect which opiates seem to possess in some instances, and iodide of potassium, in full doses of five grains every four hours, is indicated during convalescence, and blisters to the spine are also highly recommended.
Definition.—It is an infectious disease caused by the spirochetes of Obermeier, characterized by a definite febrile paroxysm which usually lasts six days, and is followed by a remission of the same length of time, then by a second paroxysm, which may be repeated three or four times.
Cause.—This disease is also known as "famine fever" and "seven-day fever." The special conditions under which it develops are similar to those of typhus fever.
|
|
|
|
|
|
|
Symptoms.—Period of incubation appears to be short and. in some cases the attack develops promptly after exposure, more frequently, however, from five to eight days. Its onset is usually abrupt, without any preliminary symptoms, and the febrile attacks, usually severe though of short duration, pass away leaving the patient comparatively well for a few days. After an interval of about a week, however, a repetition of the primary attack is experienced, and this relapse, from which the disease takes its name, may recur four or even five times.
Blood Germs.—Relapsing fever is remarkable for being the first human febrile affection of a paroxysmal character which has been definitely connected with the development of a vegetable organism in the blood. The peculiar vegetable organisms belonging to the spirochetes are found in the blood of relapsing fever patients by tens of thousands, and disappear during the temporary convalescence, to reappear with the recurrence of the febrile attack.
Symptoms Beginning.—The onset of the malady is marked by a chill or shivering-fit, severe headache, vomiting, and often jaundice; a white, moist tongue, tenderness over the pit of the stomach, constipation, enlarged liver and spleen, high-colored urine, a frequent, full and often bounding pulse, pains in the back and limbs, and frequently delirium.
Further Symptoms.—These symptoms abruptly terminate between the fifth and eighth day, as a general rule, by an exceedingly copious perspiration, and, after an interval of a week, during which it may be supposed that a new crop of the bacteria are ripening, and in which time the patient is often well enough to get up and walk about, a sudden relapse takes place, running through the same phases as the original outbreak, except, perhaps, that it is a little shorter.
At Death.—When death occurs, it is apt to happen from a fainting-fit, following excessive perspiration, or from coma, the result of suppression of the renal secretion, but as seen in America the fatality is very small, being on an average less than two per cent.
Diagnosis.—The diagnosis of relapsing fever cannot be positively made by the general symptoms during the primary onset, but may be strongly suspected, and the relapse looked for if the disease is prevailing, and exposure to the contagion has occurred. A microscopical examination of the blood during the height of the febrile movement will, however, determine the presence of the spiro-bacteria, and this investigation ought therefore always to be made.
1. Treatment.—Although so far advanced in our knowledge in regard to the vegetable nature of the true contagion of relapsing fever, we have not yet made equal progress in the specific treatment, of this complaint. The great problem, of course, is to find some mineral substance which can be taken up in the blood in sufficient quantities to check or prevent the growth of the bacteria in that vital fluid, without seriously injuring the patient himself. Quinine, so useful in intermittent fever, has proved almost worthless in this disease, and our chief reliance to reduce the high temperature is at present on cool baths or cold sponging.
|
|
|
|
|
|
|
2. For the Headache.—If the headache is very severe, dry cups to the back of the neck and along the spine may be employed, or one or two leeches may be applied behind the ears, although, since the tendency of the disease is toward great debility, it is better to avoid the abstraction of blood if possible. Opium or morphia by the stomach, or still better by hypodermic injection, is often necessary to relieve the headache and the severe pain in the limbs, and if symptoms of prostration come on early, wine or brandy must be resorted to.
3. The Urine.—A very careful watch must be maintained over the functions of the kidneys, since one of the great dangers of the disease appears to be the failure of these organs to perform their duty of purifying the blood from urea, which, when allowed by renal negligence to accumulate in the system frequently causes death by uremic poisoning. The urine should, therefore, be frequently examined, its total daily quantity noted, and the existence of albumen tested for. On account of its favorable action on the kidneys, sweet spirits of nitre in quantities of a teaspoonful every four hours is particularly applicable.
4. For the Pain.—For the muscular pains it is reasonable to expect that phenacetine, antifebrin or antipyrin will be of great service. The febrile paroxysm demands much the same treatment as typhus fever. Sponging or cold baths and nutritious and easily assimilated food.
Definition.—A fever of short duration, depending on a variety of irritative causes. A febrile movement, lasting twenty-four hours and then disappearing, may for convenience be called ephemeral fever; if of three or four days' duration, febricula.
Causes.—The most frequent cause of this form of fever is probably the ingestion of foods difficult of digestion. As a rule dyspepsia is perhaps the most frequent cause of such a fever. This is especially the case with children, where it is often spoken of as gastric fever. Another cause is exposure to cold, insufficient to produce bronchitis, tonsilitis or some other affection too slight to be recognized by the usual signs.
|
|
|
|
|
|
|
Symptoms.—The symptoms of irritative fever are those usual to fever in a mild degree, i. e., moderate elevation of temperature rarely above 103 degrees Fahrenheit, frequent pulse, flushed face, headache, sense of lassitude and weariness, loss of appetite, nausea and restlessness; in children perhaps delirium. The fever is apt to terminate suddenly by crisis on the third or fourth day.
Diagnosis.—Typhoid fever—at first the diagnosis may be impossible, but the absence of diarrhoea, tympanites, abdominal tenderness, spleenic enlargement and eruption will soon make the diagnosis apparent.
Treatment.—Absolute rest in bed, a liquid diet and repeated doses of calomel may be employed to relieve the constipation. The fever may he controlled by the following mixture:
Tincture of aconite root......................... 3 drops
Spirits of nitrous ether......................... 1/2 ounce
Acetate of liquid ammonia, add sufficient to make 3 fluid ounces.
A dessertspoonful every two hours for a child 4 years old.
Definition and Cause.—It seems necessary for the present to continue this term for a feverish process of a longer duration than febricula—a fever of long duration that is not typhoid, nor influenza—lasting from two weeks to three months and without definite lesions may be put under this head. Cases of prolonged fever succeeding pneumonia and pleurisy which subsequently recover may well be ascribed to this disease.
Symptoms are, as will be readily understood from this explanation, slight chill or chilly feelings for the initial disturbance, followed in a few hours by headache, quickened pulse, rise in temperature and constipation. Very often in persons of sensitive stomachs there is a little nausea or vomiting for twelve or twenty-four hours, and again with those of sensitive skins there may be a slight eruption of roseola, or prickly-heat, as it is often called, especially about the loins and over the back. The fever may run high enough for the overheated blood to disturb the brain and produce some delirium, especially at night; but at the end of a period, varying in duration from twelve hours to ten days, the febrile symptoms usually subside without any further derangement of the system than a very copious and debilitating perspiration, or perhaps an outbreak of the vesicles of herpes, commonly denominated "cold sores," about the face or elsewhere. Such attacks as these cause much needless anxiety, needless at least in the Northern States, to both physicians and patients, the former dreading the onset of typhoid fever or other dangerous disease, and the latter suffering an agony of suspense from which, for a time, all the knowledge of Hippocrates or AEsculapius himself could not deliver them.
|
|
|
|
|
|
|
Treatment.—The patient in these puzzling cases should be kept in bed, and allowed only light unstimulating liquid food. Cold applications may be made to the forehead and temples to relieve headache and diaphoretics combined with anodynes, such as nitre and morphia, as already directed, to reduce fever and allay restlessness: Lumps of ice are useful and refreshing to the throat when swallowed and whilst there is constipation, ripe, sweet oranges in moderation are generally safe.
Definition.—An acute infectious disease characterized by yellowness of the skin and accompanied in the severer cases by black vomit, suppression of the urine, with hemorrhage from the stomach, nose and mouth. It is almost peculiar to tropical climates and not apt to spread in temperatures below 72 degrees Fahrenheit; it is extremely fatal, perhaps, communicable from person to person and in the United States has occasionally proved itself violently epidemic.
Causes.—A hot climate, warm season, salt water, bad drainage and over-crowding favor the development of epidemics. The negro is less susceptible than the white. Strangers in an infected district are more liable to be attacked than the residents. One attack usually confers immunity from others. The exciting cause is the bacillus of Sanarelli.
Symptoms.—Yellow fever presents three well-defined stages. The first is characterized by intense pain in the head and back, injected eyes, rapid pulse and elevated temperature. This stage may last from twenty-four hours to six days—according to the severity of the attack, nausea and vomiting are present and become more intense on the second or third day. The bowels are usually constipated. As early as the first morning according to Guiteras, the face is decidedly flushed, more so than in any other infectious disease at such an early period. The second stage is characterized by the following symptoms:
The Pulse.—One of the diagnostic signs is that with an ascending temperature, there will be a descending pulse. On the first day the pulse is rarely more than 100 or 110; on the second or third day while the temperature keeps up the pulse begins to fall and may become slower to the extent of twenty beats. On the evening of the third day there may be a temperature of 103 degrees and a pulse of 75; it may, during defervescence stage, go down as low as 30.
|
|
|
|
|
|
|
The Fever.—On the morning of the first day the temperature may vary from 103 degrees to 106 degrees; during the evening of the first day and the morning of the second day the temperature keeps about the same. There is a slight diurnal variation in the second and third days.
The Calm Stage.—Third stage, the remission or stage of calm, as it has been called, is succeeded by a febrile reaction, or secondary fever, which lasts one, two or three days and in favorable cases falls by a short lysis. On the other hand, in fatal cases the temperature rises rapidly, becomes higher than in the initial fever and death follows shortly. The second stage is marked by depression of the nervous and muscular forces, and of the general and capillary circulations, slow and intermittent pulse, jaundice, urinary suppression, passive hemorrhages from the bowels, nose, gums, uterus and nearly all the organs lined with mucous membranes and, in cases of unusual severity, also from the eyes, ears and skin. Black vomit, delirium and coma generally terminate in death.
In more severe cases the symptoms resemble to a considerable extent those of relapsing fever, and it is impossible to foretell from any of these indications how serious these consequences may prove to be. In truth, these sequels constitute the most distinctive characteristics of yellow fever and comprise the "black vomit," so well known and dreaded as a fatal symptom. The black vomit is frequently preceded by the white vomit, as it is called, which is a clear acid liquid and at this time some pain is usually felt on pressure over the pit of the stomach. The occurrence of this black vomit is well known, even among sailors to West Indian ports, as a fatal sign in yellow fever, although occasionally a patient recovers after this gloomy harbinger of death has manifested itself. The yellow-jaundiced hue of the skin, when well marked, indicates a severe form of the disease, but has by no means the terribly fatal import of the black vomit.
1. Prognosis.—There are epidemics in which all persons attacked are seriously ill or die. There are epidemics of medium intensity in which the progress of the disease is limited and the mortality low. Finally, there are mild epidemics in which nearly all the patients recover. The virulence of the epidemics seems to depend upon the month in which it is imported. The pathogenic bacillus increases in virulence in the months of May, June and July. On the other hand the epidemics which are imported in the months of August, September and October are very mild owing to the attenuation of the bacillus.
|
|
|
|
|
|
|
2. The Individual Attacked.—Should the patient prior to his attack have been addicted to the use of alcohol, should he be debilitated from. over work, sexual excesses or bad living, and lastly, if he be old, the prognosis is against his recovery. The younger, the healthier and stronger the patient the greater are his chances for recovery. When the fever reaches its maximum at the onset and defervescence is continuously noted at each visit, the disease is mild; even when the fever ranges between 103 and 104.5 degrees Fahrenheit during the first three days with a remission of at least a degree in the morning and the exacerbations are less and less pronounced each night, the patient always gets well. When the fever ranges between 104 and 105 degrees Fahrenheit, still with remissions of at least a degree, but with exacerbations above the degree of fever of the previous day, the disease is to be considered grave. The cases of recovery are more numerous than the fatal ones even here. But when the fever reaches 105 degrees Fahrenheit or above within the first twelve hours the disease is usually fatal, unless heroic treatment immediately produces a defervescence of two or three degrees. Copious urine is always a good augury, even should it contain five or ten per cent. of albumen.
Scanty Urine with twenty to twenty-five per cent. of albumen on the second day, accompanying a fever about 104 degrees, indicates great danger. When the urine forms a complete coagulum on being heated death is certain. When anuria lasts twelve hours death is absolutely certain.
Intense Jaundice on the third day, urine scanty and albuminous, with black vomit occurring at the same time, always results fatally.
Black Vomit is less grave in children and in young women than in adults, particularly those over forty years of age; the latter always die.
Profuse Bleeding of the gums coming before or at the same time as the black vomit indicates an almost desperate state. Should it, however, occur on the fourth day and the gums being sound, the prognosis is less gloomy.
Women having uterine hemorrhage on the fourth and fifth days with black vomit never recover.
Treatment.—There are two great principles to be carried out in the treatment of yellow fever:
1. To strengthen and sustain the organism by fortifying the nervous system, by arresting congestion and by increasing the blood pressure and diuresis.
2. To consume, destroy and eliminate the toxin.
First of Above.—The first of the above is met by means of cold sponging by cold baths, administered, not in a routine way, but by taking the virulence of the disease and the degree of the fever as a guide.
|
|
|
|
|
|
|
Second of Above.—The second indication is met by putting the patient in a well aerated room, night and day, and making him drink in order to cleanse his blood and to dilute the toxin and eliminate them by way of the urine, two to four quarts of Vichy water in twenty-four hours.
It is during the first three days of the disease that the physician must act.
Absolute Rest.—Put the patient to bed, rest is essential and indispensable, walking, moving or the least muscular effort always increases the fever, and consequently the disease.
Aeration of the Room.—The patient must be placed in the largest and best ventilated room in the house. Exposed to the rising sun if possible. Keep the windows open night and day; do not let patient be in a draught but let the outside air enter and circulate freely.
Cleanliness.—The patient must be kept clean; should he be soiled by evacuation of the bowels or vomit, change the linen at once and plunge the soiled clothes in an antiseptic solution; cleanse the patient's teeth twice a day with cooking soda and warm water. Administer morning and night an enema containing a pint of warm water and a tablespoonful of sulphate of magnesia.
The Urine should be examined each day to see how the kidneys are acting.
Treatment of the Vomiting.—Let the patient eat small pieces of ice, but absolute rest for the stomach is the better plan.
Nourishment.—None should be given for the first seventy-two hours, after that milk every four hours. Starve your patient whether he be child or adult, unless the fever be below 103 degrees Fahrenheit. Vichy water in large quantities should be given from the onset of the disease.
Medicinal Treatment.—At the onset give one to three grains of calomel, depending on the age of the patient, but not enough to purge. In desperate cases enemas of strong black coffee to which is added two tablespoonfuls of brandy have been found beneficial.
The latest writers on yellow fever claim that the disease is spread by the mosquito. In Havana the following experiment was tried: Four men were used who had never had the disease and they were put in one room, but two were separated from the other two by a wire netting which was impervious to the mosquito. Clothes from a yellow fever patient were put into both compartments, in fact beds which had held yellow fever patients were supplied for the men to sleep on. In one compartment the mosquitoes were allowed to go in and out and the men bitten by the insects contracted the disease, but the other two men who were subjected to the same condition, minus the mosquitoes, did not contract the disease.
|
|
|
|
|
|
|
Yellow Fever and Mosquitoes.—A theory, lately come into vogue, is that yellow fever is imparted to the system by the bite of mosquitoes. The Surgeon-General of the United States has issued rules for the exclusion, by netting, of mosquitoes from houses, army tents, and so forth.
Definition.—An acute infectious disease, which is identical with the pestilence of India and the black death of Europe in former ages, and is attended with buboes or boils of the lymphatic glands of the groins, as well as other glands and occasionally with carbuncles. It is very easily communicated by human intercourse and is probably the most fatal of all the eruptive fevers.
Cause.—The specific bacillus which causes this disease was discovered by Kitasato, and occurs in the blood and in the organs of the body. It obtains entrance through the digestive and respiratory tracts.
History.—The earliest positive accounts dates from the second century of our era. From the great plague in the days of Justinian (sixth century) to the middle of the seventeenth century epidemics of varying severity occurred in Europe. Although the inhabitants of the United States have hitherto been spared any visitation from the plague, yet, as the shipments of rags from Italian ports with marble, for which they are used as wrapping is carried on quite extensively, germs of this terrible malady may at any time be imported and planted within our borders. In the last great outbreak of plague in Astrakhan, a province of southeastern Russia, the starting-point of the whole epidemic was, it is said, traced to a shawl brought by a Cossack returning from the war in Afghanistan, as part of his booty, and presented to his sweetheart. The girl wore the fatal gift for a few days, when she sickened with all the symptoms of plague and died. During the following four days the rest of her family, six in number, sickened and died. From these poor people the disease spread rapidly, and proved very fatal, devastating nineteen villages in that district. Its deadly march was only checked by a double cordon of soldiers being placed around the infected towns, and absolute non-intercourse, on the plan of the shot-gun quarantines of our Southern States, enforced.
|
|
|
|
|
|
|
Symptoms.—In the milder cases, patients are attacked with violent headache, transient shiverings, alternating with intense heat of skin, sometimes terminating in death from prostration. In the more severe form the persons affected are suddenly seized with palpitation of the heart, irregularity of the pulse, vomiting, difficulty of breathing, spitting of blood, and syncope or fainting. The face becomes pale, the expression apathetic, the eyes dull and the pupils dilated. The patients lie for three or four hours in a state of absolute prostration and then a violent accession of fever with delirium followed, in which the urine is suppressed and the bowels constipated. Dark purplish spots, from one-tenth of an inch to one inch in diameter, appear over the body, which exhale a peculiar odor somewhat resembling honey, and death is preceded by lethargy and collapse. The corpses become putrid in two or three hours after decease. Death sometimes occurs in twelve hours from the first onset.
The fever may reach 104 degrees or 106 degrees Fahrenheit, and the tongue becomes brown. The inguinal glands are most often affected, then in order, the axillary, the cervical and the popliteal. Carbuncles also develop in different parts of the skin, particularly on the legs, buttocks or back.
Treatment.—Free stimulation, nutritious food, as in the most adynamic forms of typhus and typhoid fever together with cool baths to combat the fever, are the measures indicated. Antiseptic treatment of the abscesses should be practiced.
Definition.—An infectious disease characterized by: (a) paroxysms of intermittent fever of quotidian, tertian or quartan type; (b) a continued fever with marked remissions; (c) certain pernicious, rapidly fatal forms; (d) a chronic cachexia, with anemia and an enlarged spleen.
1. Causes.—Geographical Distribution—In Europe, Southern Russia and certain parts of Italy are now the chief seats of the disease. In the United States malarial fever has progressively diminished in extent and severity during the past fifty years. From New England, where it once prevailed extensively, it has gradually disappeared. In Philadelphia and along the valleys of the Delaware and the Schuylkill rivers, formerly hot beds of malaria, the disease has become much restricted. Throughout the Southern States there are many regions where malaria still prevails, but the disease has much diminished in extent and intensity.
2. Soil Conditions.—The importance of the state of the soil in the cause of malaria is universally recognized. It is seen particularly in low, marshy regions which have abundance of vegetable growth, estuaries, badly drained, low lying districts, the course of old river beds and particularly low lying land which has been allowed to fall out of cultivation, are the favorite localities for the development of malarial fever.
|
|
|
|
|
|
|
3. Seasons.—In temperate regions, like the Central Atlantic States, there are only a few cases in spring, usually in the month of May and a large number of cases in September and October.
4. Heat.—A tolerably high temperature is one of the essential conditions for the development of the virus. It is more prevalent after prolonged hot summers.
Symptoms.—Characterized by three distinct stages of fever, chill and sweat. The paroxysm is usually preceded by a feeling of uneasiness and discomfort, sometimes languor and yawning, which forewarns the patient of its coming.
1. The Chill or Cold Stage.—Begins gradually; first there is a creep, then another, a little more severe, then another, each growing in severity until the teeth chatter and the body shakes violently. Not only does the patient look cold, but a surface thermometer will indicate a reduction of the skin temperature. The rectal temperature during the chill may be greatly increased. It lasts from fifteen minutes to an hour.
2. The Hot Stage.—Next comes the hot stage, in which all the symptoms of fever are manifested, comprising headache, nausea or vomiting, heat of skin, which may attain an elevation of 105 degrees, full strong, rapid pulse and occasionally delirium lasting from a half hour to four hours. After this follows the sweating stage, during which profuse perspiration takes place and the temperature is reduced, as a consequence, nearly or quite to the natural standard. The paroxysms, thus constituted, generally recur with considerable regularity, but may vary a good deal in different cases in regard to the interval between them.
Varieties of Ague.—The varieties of ague designated in accordance with this difference are, first, the quotidian or daily ague, in which the fit comes on usually at the same hour every day; second, the tertian ague, the most common form, when the paroxysm returns every forty-eight hours whilst the disease continues; third, the quartan, where the fit occurs every seventy-two hours, or on every fourth day; and fourth, the irregular ague, in which the fits are not distinctly periodical. Under this head is included the kind of periodical neuralgia affecting the forehead, and hence denominated brow-ague. In the quotidian form the paroxysm is apt to be the most prolonged and may last for sixteen hours out of the twenty-four, leaving of course only eight hours between its termination and the commencement of a new chill; in the tertian form, the fit is less protracted, lasting on an average about ten hours; and in the quartan it is still shorter, having an average duration of only six hours. In a fit of tertian ague continuing ten hours, we may expect to find the chill lasting from half an hour to an hour, the febrile stage, during which the patient often declares he feels as though he were burning up, extending over from three to five hours and the sweating stage occupying the remainder of the time.
|
|
|
|
|
|
|
Complications.—The most common secondary affection which occurs in the course of intermittent fever, and appears to be directly dependent upon it, is the chronic enlargement of the spleen, called "ague-cake." During the cold stage of the fit, it is probable that the spleen is always more or less distended with blood, which, being driven from the surface of the body whilst the chill lasts, finds its way to the internal organs and especially the spleen, in unusual quantity. Such congestion, if frequently repeated, seems to lead, in a majority of cases, to a real increase in amount of the structure of the spleen, and consequent enlargement of the organ.
The Ague-Cake.—The "ague-cake," when fully developed, may attain a magnitude of a foot or more in length by ten inches in breadth, and even when much smaller than this may be felt as a hard, painful and movable tumor, on the left side of the abdomen, a few inches below the heart. Such increase in size of the spleen generally indicates a rather profound impression of the malarial poison upon the system, and renders the prospect of speedy cure far less hopeful.
Lack of Blood.—Another serious complication of prolonged ague is the intense anemia, which so many persons who suffer from malarial poisoning often exhibit to a marked degree. The absence of the natural supply of good, rich, red blood gives to the skin, and especially that of the face, a dull, yellowish tint, which in malarious regions is displayed by most of the inhabitants, even the children exhibiting a pallid sallowness pitiful to behold. There is also a peculiar dejected, woe-begone expression of countenance, which is almost characteristic of malarial poisoning, and feelings of muscular weakness and fatigue on the slightest exertion are very common.
Diagnosis.—The diagnosis of ague is seldom difficult after the first paroxysm, as the regular recurrence at the same hour of the day is a feature which is so characteristic that it has given the name of "periodical fevers" to the febrile affections caused by malaria. At the first onset, it is impossible to distinguish the chill from the initial symptom of a great number of diseases, but a microscopical examination of the blood will quickly decide. The plasmodium of malaria is found in the blood during the paroxysms.
|
|
|
|
|
|
|
Treatment.—In the medical treatment of all the periodical fevers, we fortunately possess a specific of wonderful power in quinine and the other alkaloids of Peruvian bark, which have a direct control over the malarial poison, by checking the development of the bacillus malariae, which has been already referred to as being the cause of ague.
Quinine Treatment.—It is the custom to prepare the system for the administration of quinine, by the purgative action of full doses of blue-pill or other active cathartic. Give quinine in sufficient doses, during the sweating stage, to produce the slight deafness and ringing in the ears which mark the occurrence of cinchonism, as it is denominated. As a general rule, it is quite possible to do this before the time for another paroxysm, even with an attack of intermittent fever of the quotidian type. The antiperiodic must, however, in order to effect a cure, be continued in full doses of from ten to thirty grains daily, for three or four days, then reduced to half or one-third this quantity for a few days, and so persevered in for three weeks.
Preventing Fever Recurrence.—For the purpose of counteracting the tendency which intermittent fever possesses of recurring in its original violence at intervals of exactly one week, it is advisable to take the full dose of from ten to thirty grains, or whatever amount has been found to produce slight buzzing in the ears, on the sixth and seventh, the thirteenth and fourteenth, and the twentieth and twenty-first days from that on which the last chill was experienced. In this way not only the periodicity of single ague-fits, but also the periodicity of groups of the intermittent fever paroxysms, appears to be most effectually extinguished.
An East Indian Cure.—In case quinine fails or is not tolerated, other alkaloids of Peruvian bark, and preparations of the bark itself, should be fairly tried. A famous East Indian mixture for the cure of ague is Warburg's tincture, and it may be resorted to when ill-success with other forms has been met with.
Use of Peruvian Bark.—The alkaloids of Peruvian bark are, as a rule, much more efficacious in solution with some mineral acid, such as the dilute sulphuric acid.
Other Treatments.—Where for any reason Peruvian bark and its preparations fail to cure ague, the best substitute, although a far inferior one, is probably arsenic, particularly in the form of Fowler's solution, administered in quantities of five drops thrice daily, and formerly well known under the name of the tasteless ague-drop. For the cold stage, wrap the patient up well in blankets and apply hot-water bags, besides giving hot drinks. For the fever, cool sponging will relieve the patient.
|
|
|
|
|
|
|
Diet.—No particular care of the diet is requisite in intermittent fever, except to counteract as far as possible the tendency to anemia and general debility, by a liberal supply of the most nutritious food which the digestive powers are able to assimilate. In like manner, as the patient is not confined to bed, directions about nursing are unnecessary.
Prevention of Ague.—The remedy to be used in preventing an attack of malarial poisoning, when temporary residence in a fever and ague district is unavoidable, is quinine used internally, as already suggested, in doses of six or eight grains daily.
Place and Seasons.—This type of fever occurs in temperate climates, chiefly in the later summer and fall; therefore it is sometimes called estivo-autumnal fever. The severer forms of it prevail in the Southern States, where it is known as the bilious remittent fever. The entire group of cases included under the term remittent fever are bilious, remittent and typho-malarial fevers.
Symptoms.—These, as to be expected, are often irregular. In some instances there may be regular intermittent fever, occurring at uncertain intervals of from twenty-four to forty-eight hours, or even more. In the cases with longer remissions the paroxysms are longer. Commonly, however, the paroxysms show material differences; their length averages over twenty hours, instead of ten or twelve; the onset occurs often without chills and even without chilly sensations. The rise in temperature is usually gradual and slow, instead of sudden, while the fall may occur by lysis instead of by crisis. There is a marked tendency to anticipation, while frequently from anticipation of one paroxysm and retardation of another more or less continuous fever may result. In the cases of continuous and remittent fever the patient, when seen early in the disease, has a flushed face and looks ill, the tongue is furred, the pulse full and bounding, but rarely dicrotic. The temperature may range from 102 degrees to 103 degrees or go even higher.
Diagnosis.—The diagnosis of remittent malarial fever may be definitely made by an examination of the blood. The small, actively, motile, hyaline forms of the aestivo-autumnal parasite are to be found, while if the case has lasted over a week, the larger crescentic and ovoid bodies are usually seen.
|
|
|
|
|
|
|
Treatment.—The treatment of remittent fever is essentially that of intermittent fever. The continued nature of the fever and the tendency to a typhoid state demands a liquid diet, with the careful addition of stimulants.
Character.—Pernicious malarial fever differs in no respect from ordinary ague and bilious remittent, except in its greater severity. The disease is observed under three forms: First, the comatose or apoplectiform, the patient speedily loses consciousness, as though the chief force of the poison was expended upon the brain, disturbing its functions to such an extent as almost to abolish them. The fever is usually high and the skin hot and dry. Should the patient regain consciousness a second attack may come on and prove fatal.
Second Form.—In the second or algid form the symptoms of intense chill are prolonged, it may be for some hours, and death occurs in fatal cases from pure debility or asthenia, without reaction coming on. Although the patient is apathetic, the mind remains clear to the last. Vomiting and purging are the prominent symptoms, and the disease might readily be mistaken for Asiatic cholera, if it happened to occur whilst an epidemic of that malady was raging, were it not that the urine is never albuminous.
The Hemorrhagic Form.—In the third group of cases, denominated hemorrhagic malarial fever, the prominent peculiarity is bleeding, generally from the kidneys, but sometimes from the stomach, bowels, nose and mouth.
Diagnosis.—As one might expect, the blood shows marked changes in malarial fever. In the regular intermittent type there is a loss in the red corpuscle after each paroxysm, which may be considerable, but which is rapidly compensated for during the intermissions. In the estivo-autumnal fever the losses are often greater and more permanent.
Treatment.—As in the other kinds, give quinine, but in larger doses. In the case of the pernicious disease to get the effect more rapidly give quinine hypodermically as much as thirty grains at a time. Excessive care must be used to avoid abscesses.
Quinine sulphate ........................... 60 drops
Saturated solution tartaric acid............ 68 "
Distilled water to make 2 drachms.
Take 30 drops three times daily.
|
|
|
|
|
|
|
In addition to the use of quinine, stimulants must be given for the asthenia, artificial heat for the low temperature. Morphine hypodermically to relieve pain and allay nausea.
Definition.—An acute gastro-intestinal catarrh, characterized by profuse vomiting, purging and painful cramp.
Causes.—This malady, which is not contagious, occurs at times almost as an epidemic, and is occasionally fatal, so that no instance of it, however mild at first, ought to be allowed to run on without treatment. Although generally induced by indulgence in indigestible food, especially unripe fruits, there seems to be at certain seasons of the year some external influence promoting the tendency to disorder of the bowels, which is atmospheric. Especially frequent are these attacks in July and August. Cold and dampness are also regarded as predisposing agents.
Symptoms.—The primary symptoms are uneasiness at the pit of the stomach, nausea, retching and then vomiting, followed by severe watery diarrhoea, consisting of a large amount of the watery portions of the blood, and containing only a little albumen. The whole system is thus affected, in part by sympathy, but also to some extent, it is probable, by the change in the specific gravity and constitution of the blood. The attack is often abrupt, a patient being awakened out of sleep by a sudden seizure during the night. This is, however, no doubt because the preliminary uneasiness, nausea and slight colicky pains, which manifest themselves in a diurnal onset of the malady, are unfelt in the unconsciousness of profound slumber. The vomiting and purging, when once commenced, recur in rapid succession, and sometimes even simultaneously, and enormous quantities of fluid are evacuated from the system, often with the result of producing intense thirst. This thirst cannot, however, be gratified for some time, because the irritable stomach refuses to retain the smallest amount of fluid. Collapse may supervene and the skin become cold, clammy and ashen hued, the eyes sunken and the pulse frequent and feeble.
Diagnosis.—The only difficulty about the diagnosis of cholera morbus or sporadic cholera is when true Asiatic cholera is epidemic, then, if a microscopical examination of the dijecta be made, will, if it be Asiatic cholera, reveal the comma-shaped bacillus.
Treatment.—For the pain in abdomen hot applications, morphine, one-quarter grain, hypodermically; to be repeated when necessary. When the pain is less severe opium may be given by the mouth, or rectum in the form of laudanum—ten drops by the mouth, or twenty-five drops in a tablespoonful of thin starch by the rectum. When vomiting is the most troublesome symptom the following is beneficial:
|
|
|
|
|
|
|
Morphine sulphate ......................... 1 grain
Creosote .................................. 6 drops
Bismuth subnitrate ........................ 2 drachms
Mix and put into 12 papers. Take one every hour.
The prostration requires stimulants like aromatic spirits of ammonia, thirty to sixty drops at a dose or whiskey, and so forth.
Definition.—An acute infectious disease, due to the implantation of the comma bacillus of Koch, characterized by vomiting, purging, rice-water evacuations and suppression of urine.
History.—It first made its appearance in the United States in 1832. Since that time there have been several epidemics, all of which are traceable to immigration. The most serious epidemic of recent time started in India in the spring of 1892, passing from thence to Persia, Austria, Germany and Holland. A few cases reached London and New York.
Causes.—The disease-poison of cholera undoubtedly reproduces and multiplies itself during the course of the complaint, being propagated by a contagion, given off mainly, if not entirely, by the evacuations from the bowels, in which the germs of disease propagate themselves, even after their discharge, so that the stools become more virulent after they are passed, especially when mixed with water. The extended researches of Dr. Koch have proved beyond all question the existence of the cholera germ (comma bacillus) in drinking water, and traced its development in the intestines of persons who had died of the disease. The illustration in the margin shows the appearance of this cholera germ, which it is so important for every one at the peril of his life to avoid. When magnified about six hundred diameters one of the minute intestinal glands may be found to contain, as shown at a, b and c, minute bacteria or bacilli, as they are technically called, which, from their resemblance to the curved portion of a comma, but without the head of that punctuation mark, have been named the Comma bacilli. Some times these bacilli unite at their ends with their curves turned in opposite directions, so as to produce an 8 shape, or even a spiral formation.
|
|
|
|
|
|
|
This Comma Bacillus is the direct cause of cholera by its lodgment is the intestines, where it has been proved, by examination of nearly one hundred cases, to develop with great rapidity. It is easiest to detect in the earlier stages of the disease, because later on it is obscured by the development of a great many other forms of bacteria. It is distinctive of the mildest as well as of the most severe attacks, and has therefore an important diagnostic value. It is capable of successful cultivation in meat broth, in milk, on slices of potato, and especially on gelatine, in which it grows in a singular manner, producing a gradual liquefaction of the stiff gelatine around the growing colony, which sinks down into the jelly in a peculiar way. The comma bacillus thrives best at temperatures between 70 degrees and 135 degrees Fahrenheit, but is not destroyed and only has its growth checked by a cold of 18 degrees below the freezing point. It is, however, readily killed by drying, by the removal of all animal material upon which it can feed, or by acidifying the medium in which it is growing with a mineral acid. Under ordinary circumstances the bacillus when swallowed is destroyed by the gastric juice being digested in the stomach, but when there is any derangement of the stomach, from errors of diet or any other cause, so that the acid digestive liquid is deficient or absent, the bacillus escapes destruction, and may pass on into the intestine where the fluids are alkaline and it is able to develop with great rapidity. This fact in regard to the growth of the bacillus in alkaline fluids solely is one of great importance, not only in regard to the treatment of cholera, but also in connection with the subject of diet, since it is obviously highly necessary to avoid everything which, by producing indigestion, could interfere with the production of the precious gastric juice.
Modes of Infection.—In cholera epidemics we have, says Dr. Koch, instances amounting to actual experimental infection of man, as, for example, in the infection of those engaged in washing linen soiled with the discharges from the bowels of patients affected with cholera. An event of this kind is reported in the first outbreak of cholera in this country, when it was introduced into Quebec forty-two years ago.
Infection by Clothing.—Linen or other clothing soiled with choleraic discharges contains the bacilli often in a pure form, and if infection occurs through this medium it must be by the comma bacilli, frequently the only microscopic organism present, except those which are known to be innocent.
|
|
|
|
|
|
|
Infection by the Hands.—The hands of a person washing or handling such clothes may be soiled, and the bacilli introduced into the mouth by direct contact, or through the food which thus becomes contaminated, or the washing water may come in contact with the lips, and thus in some way the human being be fed with an extremely minute quantity of a pure culture of the comma bacillus.
Infection by Water.—When Dr. Koch was investigating the disease in India be observed an instance in which a certain tank furnished the water for drinking and other purposes to many people among whom the cholera was raging. He found the comma bacilli in this tank, and learned on inquiry that the clothes of the patients were washed in it. Around the tank were some thirty or forty huts inhabited by upward of two hundred people, and of these persons seventeen died, whilst the number of those taken sick was not ascertained. The tank in this case also received the refuse from the dwellings. In fact, it is common in India for the Hindoos to bathe in the tank which affords their water-supply, to wash their utensils in it, to deposit their excrement upon its bank, and if a hut has a latrine, or substitute for one, its outflow is apt to be into the tank. In this particular instance it was found, after a time, that the bacilli became less abundant in the tank-water, and coincidentally the cholera declined among the inhabitants of the huts along its shore. Here, if the epidemic had been the cause of the bacilli, instead of the result of their development, the number of these minute organisms ought to have been augmented after the disease began to be less violent. For further dissemination of the disease, the cholera discharge must be retained in a moist state, since complete drying seems to destroy the poisonous property of the virus; and this view is sustained by what we have long known in regard to the spreading of cholera by contaminated water-supply, or more directly by soiled hands, or even conveyance by insects, as, for example, by blow-flies alighting upon meat and other food. Drains may be infected, and through them the drinking water polluted; but as the virus cannot preserve its activity in a dry state little can be hoped for from aerial disinfection, nor does it seem probable that, except under certain conditions of unusual moisture can cholera be transmitted by merchandise or by letters, even if the latter are not disinfected, but only by human intercourse.
|
|
|
|
|
|
|
Symptoms.—Period of incubation ranges from two to five days. The symptoms of cholera commonly present themselves sufficiently gradual to admit of arrangement into three distinct groups or stages:
1. Preliminary Diarrhoea.—This may set in abruptly without any previous indications. More commonly there are for one or two days colicky pains in the abdomen, with looseness of the bowels, perhaps vomiting, with headache and depression of spirits. As a rule the temperature is not elevated.
3. The Stage of Collapse.—Spasmodic griping pains are felt and depression of the powers of circulation and respiration come on, attended with a sense of faintness and oppression over the heart, whose beat at times is hardly discernible, and the pulse at the wrist may be absent. Copious purging, at first of the contents of the intestines, and afterward of a thin, watery fluid, resembling water in which rice has been washed, having an alkaline reaction, and sometimes tinged red with blood, soon commences, and is usually accompanied with violent vomiting and a sensation of burning heat in the stomach. In a short time, perhaps within a few hours, there results from this excessive drain upon the circulation, coldness and dampness of the whole surface of the body, lividity of the lips, cold breath, an unquenchable thirst, a feeble rapid pulse, difficult respiration, with extreme restlessness, and suppression of the secretion of the kidneys.
Symptoms in Fatal Cases.—In fatal cases are noticed blueness of the whole body, the sunken and horror-stricken countenance denominated the Hipprocratic face, popularly known as the appearance of being struck with death, and a peculiarly suppressed voice, this condition ending either immediately in fatal collapse or in reaction followed by violent secondary fever.
3. Stage of Reaction.—This is characterized by return of warmth and colds, the latter more slowly and the reestablishment of secretions. Especially favorable is the return of the urinary secretion. Along with these changes the vomiting and purging occur at longer intervals. The heart's action becomes stronger, and there are no abdominal pains. Not infrequently this favorable condition is interrupted by a recurrence of a severe diarrhoea, and the patient is carried off in a collapse. Other cases pass into a condition of what has been called cholera-typhoid, a state in which the patient is delirious, the pulse rapid and feeble and the tongue dry. Death finally occurs with coma. These symptoms have been attributed to uramia.
Diagnosis.—The only affection with which Asiatic cholera could be confounded is the cholera morbus, which occurs as a rule during the summer months, of which mention has been made.
|
|
|
|
|
|
|
Preventive Measures.—Preventive measures are all important, and isolation of the sick with thorough disinfection have effectually prevented the disease from obtaining a foothold in either the United States or in England.
The course of cholera during the last epidemic which visited the United States, and ravaged the Mississippi Valley in 1873, reaffirmed the lessons of previous outbreaks of this disease abroad. This was especially the case as regards the supreme importance of pure water-supplies in cities and villages, all of which should be boiled before using, and of having all wells and water-springs which are used by the people effectually guarded against any possible soakage and contamination from privies and other sources of defilement by excrement. It must be admitted that the history of outbreaks of cholera, in all parts of the world, conspicuously illustrates the vital importance of procuring all supplies of drinking-water from sources which cannot become polluted by the soakage into them of intestinal discharges, or from outflowings in any such way as to be carriers of bowel-diseases, particularly not of cholera and typhoid fever. The story of the Broad street pump in London, which killed five hundred people in one week during the last great cholera epidemic, and was found to have its water contaminated by soakage of cholera evacuations from an adjoining cess-pool, has already been related (see Book III), but it should be retold to every one as a terrible warning against the almost universal dangers of water-pollution. An item in the London Lancet, printed in 1882, states that a recent analysis of the water of the Holy Well of Mecca, which is so eagerly drunk by the pilgrims, as a part of their religious rites, shows the water to be sewage, about ten times stronger than the average London sewage. And during the same month that this report was given, came the news that the cholera had made its usual annual appearance among the pilgrims to the shrine of Mahomet in the Holy City of Mecca. It therefore appears extremely probable that by suitable investigation of the water of the Holy Well, there might be found in it a perennial supply of the cholera germs, and such a demonstration of the true origin of the frightful cholera epidemics which, spread by the caravans of returning Moslem pilgrims, have so often devastated large sections of Europe and Asia, would be a triumph for experimental hygiene of which the whole world of science might be proud.
The impurity of the local atmosphere of a dwelling, a village, or a particular district, is proved to be a matter also of public concern, and environed in a polluted atmosphere, the palatial mansions of wealth and gayety may suffer equally with the tenements of the humblest classes. The specific migratory power of cholera, whatever its nature, has the faculty of infecting districts in a manner most detrimental to health only when the atmosphere is fraught with certain products, susceptible under its influence of undergoing poisonous transformations. Through the unpolluted atmosphere of cleanly districts it migrates perhaps without a blow because that which it can kindle into poison is not there.
|
|
|
|
|
|
|
Disinfection.—1. The vomited matter and the discharges from the bowels are to be gathered and put in a carbolic solution one to twenty, or chlorinated lime one to ten, some of which should be in the vessel before it is used. In the country where the excreta can be thrown in a pit, "whitewash" is a cheap disinfectant.
2. After vomiting the mouth of the patient should be rinsed with a solution of hydronaphthol one to five thousand, care being taken that none of it is swallowed. After each evacuation from the anus the buttocks and thighs should be washed with soap and water.
3. All body and bed linen soiled with the discharges should be immediately moistened with a carbolic solution one to sixty, removed from. the apartment in a covered vessel and boiled for one-half hour in a one per cent. solution of washing soda.
4. Napkins, towels, and so forth, should be treated in like manner.
5. All dishes, knives, forks, spoons, and so forth, after each meal, should be boiled for the same length of time in the same medium.
6. The remains of meals should be thrown in whitewash and removed at the end of each day.
7. Door knobs are liable to be soiled by the hands of one carrying out the excreta and should be carefully watched.
8. In cases of death the body, without being washed, should be wrapped in sheets wet in a solution of bichloride of mercury and should be buried promptly.
Directions for Nurses.—1. Nurses should not hold any direct communication with others while in attendance on the case.
2. They should under no conditions take their meals in the same room with the patient. After touching the patient her hands should be washed in bichloride of mercury one to one thousand.
3. The teeth should be cleansed after each meal, as the mouth affords a peculiar favorable nidus for decomposing matter and would therefore, be favorable for the growth of the cholera bacillus.
Treatment.—The successful treatment of cholera depends largely upon how promptly remedial measures are commenced, for if the first sign of relaxation of the bowels is met at once by an energetic astringent and opiate, such as the mixture of a teaspoonful of syrup of galls, ten drops of laudanum, and one drop of chloroform, repeated every hour if necessary, or a compound of ten drops each of tincture of camphor, of capsicum and laudanum, to which, if there is any vomiting, five grains of bismuth should be added, it is certain that many lives might be directly saved by medical treatment. External applications of heat should be made, warm applications to the abdomen will be found grateful to the patient. Sometimes a pill of opium and acetate of lead, with a little capsicum, using, for example, one-half of a grain of opium, two grains of the sugar of lead, and a quarter of a grain of cayenne pepper, is singularly serviceable, and being carried in small compass is especially convenient for travelers.
|
|
|
|
|
|
|
Pain Treatment.—Should the pain be great control it with one-fourth grain injections of morphine hypodermically. As owing to the profuse discharges the blood is very much concentrated, subcutaneus injections of normal salt solution should be given.
The following well-known cholera or diarrhoea mixture is of great value in the early stages:
Tincture opium .................................. 1 ounce
Spirits of camphor............................... 1 "
Tincture capsicum ............................... 1 "
Pure chloroform ................................. 3 drachms
Alcohol sufficient to make 6 ounces.
Mix and take one teaspoonful every one or two hours,
Definition.—An acute infectious disease due to Klebs-Loefler bacillus, characterized by a local fibrinous exudate usually upon the mucous membrane of the throat, with a moderate fever, glandular enlargements and great prostration.
Cause.—The disease is endemic in all large cities, and becomes epidemic at times; while other contagious diseases have diminished in the past decade, diphtheria has increased, particularly in cities.
Contagiousness.—Diphtheria is a highly contagious disease and is readily transmitted from person to person. The bacilli may be received from (1) discharges of diphtheria patients, (2) from the secretions of the nose and throat of convalescence cases, in which the virulent bacilli persists, (3) from the throats of healthy individuals who have acquired the bacilli from being in contact with others having the virulent bacilli on their persons or clothing.
|
|
|
|
|
|
|
Dangers of the Disease.—No disease of temperate regions proves more fatal to physicians and nurses. There seems to be particular danger in examining and swabbing out the throat; for in the gagging, spluttering and coughing efforts the patient may cough mucus and flakes of membrane into the physician's throat. The bacillus attaches itself to the bedding, clothes and room of the patient with great tenacity.
Attack Upon Children.—Very young children are rarely attacked, the age of predilection being from the second to the fifteenth year. The greatest number of deaths occurs between two and five years of age. Girls are attacked in larger numbers than boys. Adults are frequently affected.
Symptoms.—Period of incubation is from two to seven days; oftener two (Tyson).
According to the location we may speak of the pharyngeal, laryngeal and nasal varieties.
1. Pharyngeal.—The symptoms are those of an ordinary febrile attack. Slight chilliness, fever and aching pains in the back and limbs, usually the temperature rises in the first twenty-four hours to 102 degrees to 103 degrees Fahrenheit. There is a slight redness and feeling of soreness in the throat, generally upon one or both tonsils, and on careful examination the tonsils and adjacent portions of the fauces are found to be a little swelled. A whitish-gray patch of false membrane, looking at first like a small ulcer in the mucous surface, next makes its appearance, and this may spread until, by the third day, it has covered the tonsils, fauces and perhaps the uvula.
The False Membrane.—If this false membrane is forcibly torn away, as, for example, by some of the various forceps which were at first invented for the purpose, a raw bleeding surface is exposed, which in a few houra is again covered with a new growth of the layer of membrane. This structure, which is partly composed of an exudation of lymph and partly of a fungoid growth, the micrococcus diphtheriticus, quickly undergoes putrefactive changes, together with the outer layer of mucous membrane lying immediately beneath it, so that there is often a superficial ulceration, from which an unhealthy discharge flows, and a putrid odor frequently emanates constantly, in severe cases of diphtheria.
Thickness of the Membrane.—The thickness and density of the false membrane varies greatly in different cases, and in different epidemics. Sometimes it is scarcely thicker than writing-paper, and has hardly more consistence than thick cream. At other times it is firm and tough, almost like leather, and may even attain the thickness of a quarter of an inch. Although in mild cases and those of moderate severity, its color is grayish-white, in debilitated states of the system, and when there is a tendency to bleeding from the throat and other mucous surfaces, it may be tinged, probably by the altered blood elements of a yellow, yellowish-brown, or dark-brown hue.
|
|
|
|
|
|
|
Diagnosis.—(a) There may be no local manifestation of the membrane, but a simple catarrhal angina, associated sometimes with a croupy cough. The detection in these cases of the Elebs-Loefler bacillus can alone determine the diagnosis.
(b) There are cases in which the tonsils are covered with a pultaceous exudate, not a consistent membrane.
(c) Cases which begin and often run their entire course with the local picture of a typical lacunar amygdalitis, they may be mild, but in other cases there is a rapid development of membrane and extension of the disease to the pharynx and nose with septic and constitutional symptoms.
2. Nasal Diphtheria.—In membranous or fibrinous rhinitis, a very remarkable affection seen usually in children, the nares are occupied by thick membranes, but there is entire absence of constitutional disturbances. Ravenel collected seventy-seven cases, all of which ran a benign course, and in all but a few the membrane was limited to the nose and the constitutional symptoms were slight or absent. On the other hand nasal diphtheria is apt to present a most malignant type of the disease, high fever, marked glandular evolvement and great prostration by epistaxis and by excoriation of the lips.
3. Laryngeal Diphtheria.—The affection begins like an acute laryngitis, with a slight hoarseness and rough cough, to which the term croupy has been applied. After these symptoms have lasted a day or two, with varying intensity, the child suddenly becomes worse, usually at night, and there are signs of impeded respiration.
Difficulty of Breathing.—At first the difficulty in breathing is paroxysmal, owing probably to a spasm of the muscles of the glottis. Soon the dyspnoea becomes continuous, inspiration and expiration become difficult, particularly the latter. The voice is husky and is reduced to a whisper. The color gradually changes and the imperfect aeration of the blood is shown in the lividity of the lips and finger tips. Restlessness comes on and the child tosses from side to side, vainly trying to get breath. Occasionally in severer paroxysms portions of the membrane are coughed up.
The Fever.—The fever is rarely very high, and the condition of the child at the onset is good. The pulse is always increased in frequency. In favorable cases the dyspnoea is not very urgent, and the color of the face remains good. In unfavorable cases the dyspnoea becomes more and more urgent, the cyanosis deepens, and the child, after a period of restlessness, sinks into a semi-comatose state, and death finally occurs from poisoning of the nerve centres by carbon dioxide.
|
|
|
|
|
|
|
1. Complications.—Hemorrhages from the nose or throat may occur in severe ulcerative cases. Skin rashes are not infrequent. In very bad cases, with extensive sloughing, the septic particles may reach the bronchi and excite gangrenous processes, which may lead to severe and fatal hemorrhages.
2. Renal Complications.—These are common, albuminura is present in all severe cases; nephritis may set in quite early in the disease; it sets in at times with complete suppression of the urine.
3. Paralysis.—This is rather frequent, occurring in from ten to even twenty per cent. of cases.
Diagnosis.—The onset is more sudden than in scarlet fever, the fever higher, the pulse more rapid and the tongue presents a strawberry appearance. For the rest of the diseases it is sufficient to state that, for the purpose of insuring proper sanitary precautions, it is advisable to consider all cases of sore throat, with fever and prostration of strength, in which patches of false membrane, however small, appear upon the tonsils or fauces, as diphtheritic in their character. All cases should be treated as diphtheria until the contrary is proven.
Preventive Measures.—Recent investigations having proved that the poison of diphtheria is portable, communicable by infection, and capable of reproducing itself outside of the human body, diphtheria must now be ranked as both a contagious and infectious disease. The following rules are therefore more imperative than ever before:
1. When a child or young person has a sore throat, a bad odor to its breath, and especially if it has fever, it should immediately be separated and kept secluded from all other persons, except necessary attendants, until it be ascertained whether or not it has diphtheria, or some other communicable disease.
2. Every person known to be sick with diphtheria should be promptly and effectually isolated from the public. Only those persons who are actually necessary should have charge of or visit the patient, and these visitors should be restricted in their intercourse with other individuals. Children residing in a house where there is a case of diphtheria should not be permitted to attend school.
|
|
|
|
|
|
|
3. When a case of diphtheria is fully developed, the same precautions in regard to free ventilation, disposal and disinfection of discharges, bed or body linen, and so forth, isolation during convalescence (or management of the corpse should death unfortunately occur), and so forth, ought to be enforced which have already been recommended in regard to small-pox and cholera.
4. It is particularly important that persons whose throats are tender or sore from any cause, should avoid possible exposure to the contagion of diphtheria. Children under ten years of age are in much greater danger of taking the disease, and after they do take it of dying from it, than are grown persons. But adults are not exempt, and mild cases in them may cause whole series of fatal attacks among children.
5. Numerous instances are recorded where the contagion of diphtheria has retained its virulence for weeks or months, in cesspools, heaps of decaying vegetable matter, damp walls, and so forth, and been carried for long distances in clothing, in sewers, in waste pipes from stationary washstands, and in other conduits. Hence all sewer connections and other carriers of filth should be well ventilated and disinfected, and children particularly should not be allowed to breathe the air of any water-closet, cesspool, or sewer into which discharges from patients sick with diphtheria have entered, nor to drink water or milk which has been exposed to such air or the atmosphere of the sick-room.
6. Beware of any person who has a sore throat; do not kiss such a person or take his or her breath; do not drink from the same cup, blow the same whistle, nor put his pencil or pen into your mouth.
1. Treatment.—Local treatment—germicides and disinfectants are best applied when possible by the spraying apparatus at intervals of an hour, or at most every two hours. If the spray can not be used, as is often the case with children, a soft sponge may be used. The most satisfactory solution for this purpose is equal parts of peroxide of hydrogen and Dobell's solution. Carbolic acid may be used in the proportion of fifteen drops to an ounce of glycerine and water. Boric acid in saturated solution is fairly good. Where there is the laryngeal form the patient should breathe an atmosphere saturated with the vapor of slacked lime.
2. Constitutional Treatment.—For checking the growth of the membrane the preparations of mercury are good. The bichloride of mercury in dose of one-forty-eighth to one-twelfth (Tyson) for an adult, in conjunction with the tincture of the chloride of iron and chlorate of potassium every two hours. These doses are given to adults, and they need not be much reduced for children. Quinine should form part of the medical treatment in doses of from ten to twenty-four grains in twenty-four hours.
|
|
|
|
|
|
|
Diet.—Stimulating, nourishing and easily assimilated food is necessary. Milk is preferred to all else, fortified with full doses of whiskey, two drachms to an ounce being required in all severe cases. Milk may be alternated with animal broths. When deglutition is difficult nutrient enematas may be given, for this peptonized milk is best.
Opening the Windpipe.—When laryngeal obstruction is imminent intubation or tracheotomy should be performed. Lives have been saved by both these operations. Such cases should breathe air charged with vapor of lime.
3. Serum Treatment.—It has been fully demonstrated that antitoxin or the serum of immunized animals, is the best therapeutic agent in diphtheria. The investigation conducted by the American Pediatric Society has shown that the mortality under the serum treatment in 5, 794 cases was only 12.3 per cent. The strength of the serum is measured in units, the latter being equal to 1 c.cm. of "normal serum," which is the blood serum of an immunized animal so active that one-tenth of a c.cm. will antagonize ten times the minimum of diphtheria poison fatal to a guinea pig weighing 300 grams. For children over two years old the initial dose should be from 1,500 t� 2,000 units in all severe cases, including those of laryngeal stenosis; this dose to be repeated in from eighteen to twenty-four hours if there is no improvement seen, and again in twenty-four hours if the course of the disease is unfavorable. The third dose is rarely necessary. Mild cases should receive 1,000 units for the first injection, a second is rarely necessary. In cases injected during the first two days the mortality is less than 5 per cent. The question of immunizing those exposed to the disease is a very practical one. It has been carried out on a very large scale in some institutions with satisfactory results. The immunity is only transient and only persists for a few weeks.
For full description and treatment of this disease see Part XII, DISEASES OF CHILDREN.
For full description and treatment of this disease see Part XII, DISEASES OF CHILDREN.
|
|
|
|
|
|
|
Definition.—An acute infectious disease, appearing at irregular intervals, characterized by extraordinary rapidity of extension and the large number of people attacked.
Causes.—It is caused by the bacillus of Pfeiffer. It spreads with remarkable rapidity. In the large pandemic of 1889-1890 some of the large prisons escaped entirely. The outbreaks of the epidemics are independent of all seasons and meteorological conditions, though the worst epidemics have been in the colder seasons of the year. One attack does not protect. A few persons do not appear liable to the disease.
Symptoms.—Incubation is from one to four days. The onset is usually abrupt, with fever and its associated phenomena. Usually there is coryza and sneezing, with or without watering of the eyes. No age is exempt, as it attacks with impunity the infant as well as the old man. There is generally a cough, to which is added very soon profuse expectorations.
Expectorations.—The cough may be paroxysmal, with prostration at the end of the spell. It often persists, while the bronchitis may pass into broncho-pneumonia, or a croupous-pneumonia may supervene. Another mode of onset is by extreme and sudden prostration. This prostration is apt to be prolonged even in mild cases far beyond what seems reasonable.
Mental Depression.—This is a frequent symptom, and suicide has been its terminal act. There is always more or less fever, ranging from 101 degrees to 106 degrees Fahrenheit. Delirium is nearly always associated with a high fever.
Nausea and Vomiting.—With the onset of the fever there may be nausea and vomiting, or the attack may set in with abdominal pains, profuse diarrhoea and collapse.
Diagnosis.—During a pandemic the cases offer but slight difficulty. The profoundness of the prostration, out of all proportion to intensity of the disease, is one of the most characteristic features.
Treatment.—Isolation should be practiced if possible. Old people should be guarded against all sources of infection. The secretions, nasal and bronchal, should be disinfected. In every case the disease should be regarded as serious and the patient kept in bed until the fever has completely disappeared. From the onset the treatment should be supporting, and the patient should be well fed and nursed. At night ten grains of Dover's powder may be given. At the onset a warm bath is sometimes grateful in relieving the pains in the back and limbs. If there is much fever and delirium small doses of antipyrin may be given and an ice-cap applied to the head. In cases with great cardiac weakness stimulants should be given freely and during convalescence. Strychnia in full doses and good, nutritious diet, cheerful surroundings and change of air are essential. The depression of spirits following this disease is one of its most unpleasant and obstinate features.
|
|
|
|
|
|
|
Definition.—An acute infectious disease, usually commencing with a specific inflammation of the mucous membranes of the nose and throat, and originating in contagion derived from a glandered horse, ass or mule, and characterized by the appearance of vesicles in the mucous membrane of the mouth and between the toes and nodules beneath the skin; in the latter it is called farcy.
Cause.—The disease belongs to the infective granulomata. The local manifestations in the nostrils and skin of the horse are due to one and the same cause. Man becomes infected by contact with diseased animals, and usually by inoculation on an abraded surface of the skin. The contagion may also be received on the mucous membrane.
Symptoms.—The disease has an incubation of from three to five days. At this time there is a febrile movement, with malais and loss of appetite. On the mucous membrane of the lips and tongue and sometimes on the hard palate come vesicles containing a yellowish serum. There is a sensation of heat and burning through the mouth, and the swelling may be so great as to make speech difficult and swallowing painful. There is copious salivation. Almost simultaneously appear vesicles between the fingers and toes and around the nails.
Treatment.—If seen early the wound should be either cut out or thoroughly destroyed by caustics and an antiseptic dressing applied. In the acute cases there is very little hope. In chronic cases recovery is possible, though often tedious.
Definition.—An acute infectious disease of animals, due to the bacillus anthracis, especially affecting cattle and sheep, but transmissible to man.
Causes.—It is very prevalent in Europe and Asia, but is rare in this country. A protective inoculation, with a mitigating virus has been introduced by Pasteur. In animals the disease is conveyed sometimes by direct inoculation, as by the bites and stings of insects, by feeding on the carcasses of animals which have died of the disease, but more commonly by feeding in pastures in which the germs have been preserved. Pasteur believes that the earth worm plays an important part in bringing to the surface and distributing the bacilli which have been propagated in the buried carcass of an infected animal. Certain fields or even farms may thus be infected for an indefinite period of time.
|
|
|
|
|
|
|
Symptoms,—Anthrax lias a period of incubation of about one week, after which there are a number of modes of manifestation of the disease.
1. External Anthrax or Malignant Pustule.—This occurs most frequently on the exposed surfaces, the arms, face or hands, and produces in a few hours a slight redness like that from a mosquito bite, and afterward a little blister. This is soon succeeded by a spreading hardness of the surrounding tissues, which mortify and turn black. Crops of secondary vesicles appear, the neighboring lymphatic glands become inflamed, the breath grows fetid, and there is thirst, high temperature and frequent pulse, and death may take place in from twelve to forty-eight hours, with all the symptoms of profound blood-poisoning. Occasionally recovery takes place, but it is only in mild cases, in which all the symptoms, local and general, are less severe; the vesicles dry up into scabs and the hardness passes away.
2. Malignant Anthrax, Edema.—This form begins in the eyelid, and from thence passes into the head, arms and hands. It is characterized by the absence of the vesicles and by the most extensive edema, which may follow, rather than precede, the constitutional symptoms. The most fatal cases are seen when inoculation takes place about the head and face. A feature in both these forms of malignant pustule, to which many writers refer, is the absence of feelings of distress or anxiety on the part of the patient, whose mental condition may be perfectly clear. He may be without apprehension, even though his condition is very critical.
Diagnosis.—Diagnosis can be readily made from the character of the lesion and the occupation of the patient. When in doubt a microscopical examination of the fluid from the pustule may show the presence of the bacillus.
3. Intestinal Form.—In these cases the infection is usually through the stomach and intestines and results from eating the flesh or drinking the milk of diseased animals. It may, however, follow an external infection if the germs are carried to the mouth. In acute cases there are dyspnoea, cyanosis, great anxiety and restlessness, and toward the end convulsions or spasms of the muscles.
|
|
|
|
|
|
|
4. Wool Sorters' Disease.—This important form of anthrax is found in large establishments in which wool or hair is sorted and cleansed. The hair and wool imported into Europe from Russia and South America appear to have induced the largest number of cases. Many of these show no external lesion. The infected material being swallowed or inhaled with the dust.
Symptoms.—There are rarely any preliminary symptoms. The patient is seized with a chill, becomes faint and prostrated, has pains in the back and legs and the temperature rises to 102 degrees or 103 degrees Fahrenheit. The breathing is rapid, and there is much pain in the chest. There may be a cough and signs of bronchitis. There may be vomiting, and death may occur within twenty-four hours. In more protracted cases there may be diarrhoea, delirium and unconsciousness.
Treatment.—In malignant pustule, the site of inoculation should be destroyed by the caustic or hot iron and a little powdered bichloride of mercury sprinkled over the exposed surface. The local development of the bacilli about the site of inoculation may be prevented by the subcutaneous injections of carbolic acid or bichloride of mercury. The injections should be made at various points around the pustule, and may be repeated two or three times a day.
Internal Treatment,—The internal treatment should be confined to the administration of stimulants and plenty of nutritious food. Davies-Colley advises ipecacuanha powder in doses of five to ten grains every three or four hours. In the malignant form, particularly the intestinal variety, little can be done. Keep the bowels active.
Definition.—This is a specific, contagious inflammation of the skin, tending to spread over large portions of the cutaneous surface with the usual signs of inflammation—pain, heat, redness and swelling.
Causes.—This complaint has, as a rule, for its starting point some slight wound or abrasion of the skin, although occasionally it seems to arise spontaneously, affecting the head and face in such instances more frequently than any other portion of the body. It is particularly prevalent in the spring of the year. It can be conveyed by a third person. The poison certainly attaches itself to clothing, furniture and bed-room walls. Recently delivered women and persons who have been the subjects of surgical operations are particularly susceptible to it.
Predisposing Causes.—Predisposing causes are Bright's disease, alcoholism and debility. The specific agent of the disease is a streptococcus growing in long chains, the streptococcus erysipelatous.
|
|
|
|
|
|
|
Symptoms.—Period of incubation is variable from one to eight days. The stage of invasions is often marked with a rigor and followed by a rapid rise in temperature and other signs of an acute fever, when there is a local abrasion, the spot is slightly reddened, but if the disease is idiopathic there is seen within a few hours a slight redness over the bridge of the nose and on the cheeks. The swelling and tension of the skin increase and within twenty-four hours the external symptoms are well marked.
The Skin.—The skin is smooth, tense and edematous. It looks red, feels hot and the superficial layers of the skin may be lifted as small blebs. The swelling increases rapidly, and during the second day the eyes are usually closed.
Further Symptoms.—The first affected parts gradually become pale and less swollen as the disease extends. When it reaches the forehead it progresses as an advancing ridge, perfectly well defined and raised; and often on palpation hardened extensions can be felt beneath the skin, which is not yet reddened. Even in cases of moderate severity the face is enormously swollen, the eyes closed and the lips edematous, the ears thickened, the scalp is swollen and the patient's features quite unrecognizable.
Blood Poisoning.—The lymphatic vessels and glands, especially the cervical, are almost always more or less affected, and poisoning of the blood as in pyemia not infrequently occurs. One attack of the disease, so far from affording any protection, generally leaves the patient particularly susceptible to the malady for a long time, perhaps for life. Delirium is present, the tongue becomes dry, the pulse feeble and there is marked tendency to death from toxema. In the majority of cases, however, even with extensive lesions the constitutional disturbances, considering the height of the fever range, is slight.
Treatment.—Isolation must be carried out. A practitioner in attendance on a case of this disease should not attend a woman in confinement. The disease is self limited and a large majority of cases get well without any internal medication.
Diet.—The diet should be nutritious and light. Stimulants are not required, except in the old and feeble. For sleeplessness, restlessness and delirium chloral and the bromides may be given, or if these fail, opium, when the fever is high the patient may be bathed or sponged. Of the internal remedies the tincture of the perchloride of iron has been highly recommended.
|
|
|
|
|
|
|
Local Treatment.—For the local treatment, two per cent. solutions of carbolic acid, the corrosive sublimate solution 1 to 2,000. In the Polyclinic Hospital in Philadelphia the application of ichthyol ointment over the reddened area, and should there be a wound, washing it out with normal salt solution have proved very efficacious.
Definition.—It is a condition in which, with or without a local site of infection, there is a microbic invasion of the blood and tissues, but in which there are no foci of suppuration.
Symptoms.—Illustrative cases of the more usual form of septicemia are puerperal fever, following a retained placenta, infection by scarlet fever, or difficult labor involving lacerations and the poisoning by a dissecting wound. The symptoms set in from three hours to four days, usually twenty-four hours.
Initial Symptoms.—The usual initial symptom is a chill varying in severity; it may, however, be preceded by a headache and malaise and is always followed by a high fever. In bad cases the chill is repeated daily and the temperature rises high. I have known of one instance in which it went to 106.7 degrees Fahrenheit. The patient is restless, the tongue at first red and glazed becomes dry and leathery, the pulse at first full and bounding becomes weak and compressible with a rate of 130 or more. Prostration is marked.
The Fever.—The fever is subject to remissions which give rise to the inexperienced to delusive hope. The chill is followed by profuse sweating and further prostration, the mind early begins to wander and delirium of the low muttering kind is soon established. There is a tenderness over the abdomen in puerperal cases and in all a tendency to enlargement of the spleen with hypostatic congestion of the lungs and often broncho-pneumonia will result.
Diagnosis.—This is usually easy, the resemblance of the more serious form to intermittent fever has been referred to. In this disease the remissions are not so total and the patient remains very ill.
Treatment.—In treatment all possible infecting foci should be removed by surgical methods; after this the strength should be supported by quinine, strychnine and stimulants. The food should be liquid and of the most nourishing kind. The fever should be reduced with cold sponging.
|
|
|
|
|
|
|
Definition.—Pyemia is a general febrile affection due to sepsis, characterized by recurring chills and profuse sweats with remissions or intermissions in the fever, also by abscesses variously disseminated in the different tissues and organs of the body.
Causes.—The same essential cause lies at the bottom of pyemia as of septicemia, but associated with this disease are the important etiological factors, thrombosis and embolism. Fragments of a venous thrombus due to a phlebitis at the seat of putrid inflammation are broken off and carried in the circulation until a lodgment is effected. These fragments swarm with bacteria and the embolus excites intense inflammation, which goes on to abscess formation. The emboli may be multiple, and there will be as many abscesses as there are emboli. The seats of election are lungs, liver, spleen, kidneys, brain and joints and the various connective tissues in the order above given.
Other Causes.—Other causes are gunshot injuries of bone and compound fractures, gonorrhea and prostatic abscesses.
Symptoms.—A rapidly rising fever, often so closely followed by a chill, that its previous existence is often not suspected. The severity of the chill is proportionate to the intensity of the infection. The temperature during the chill reaches 103 degrees to 105 degrees Fahrenheit, and is followed by a sweat and fall in temperature, after which the latter rises again to a point even higher than was at first attained. The temperature may rise and fall several times, but as a rule each one goes higher than the preceding one.
Other Symptoms.—The other symptoms of fever are also present, thirst, loss of appetite and nausea. The strength of the patient rapidly wanes and he soon sinks into a condition of exhaustion and semi-consciousness from which he may be aroused to take medicine and nourishment.
Diagnosis is not usually difficult, a careful study of the case will show marked differences in history to typhoid fever and malarial fever. There are no rigors followed by sweats in typhoid, and finding the plasmodium malarias in the blood of suspected patient will settle the case should it be malaria.
Treatment is like that of septicemia. Remove the foci of infection surgically, and after that the symptoms are to be combated and the strength supported to the utmost.
This page is maintained by
Charles Keith.
Contact:
Send me a message
Last Modified: Monday, 13-May-2013 15:31:46 EDT