|
|
|
|
|
|
|
Bacteriology.—Bacteriology is the science which treats of germs. Their discovery within a few decades has wrought a revolution in surgical treatment. No intelligent understanding can be had of the principles of surgery without at least some elementary knowledge of bacteriology. For its more complete discussion see the special article upon the subject.
Micro-Organisms, Germs, Bacteria or Microbes are minute, vegetable cells, most of which can be seen by the microscope only. They are widely distributed, being in the air we breathe, food, water, in the soil, on vegetable and animal matter either living or dead. They form a microscopic flora, a vast vegetable world, with varieties probably as innumerable as the vegetation with which we are so familiar. Some microbes when introduced into the system are non-disease producing, harmless. Others are pathogenic or disease producing, most virulent in their action.
Yeasts include several species of germs, the action of which, in bread raising and in producing alcoholic fermentation, is familiar. They are, for the most part, harmless to the human system; one variety, however, grows upon the mucous membrane as thrush.
Molds represent another class, familiar to us in their growth upon old leather and upon stale bread.
Bacteria.—The sub-class of germs known as bacteria are the ones of chief interest to the surgeon. Of the three forms, coccus, berry-shaped or round; bacillus, rod-shaped, and spirillum, corkscrew-shaped; the latter plays no role in surgery.
Growth of Bacteria.—Bacteria may multiply with amazing rapidity. Under ideal conditions a single cell in one day will have sixteen million descendants, and in three days the mass of new cells would weigh 7,500 tons. Multiplication is chiefly by subdivision, one cell dividing into two, the two into four and so on; or by "seeds," called spores.
|
|
|
|
|
|
|
Soil for Bacteria.—They require a suitable substance or "soil." Some grow better upon living matter, others upon dead. Most of them are readily grown artificially upon the blood serum of an animal, a suggestion as to the favorableness of the human tissues for a soil. They need heat and require water. Most grow better when exposed to the oxygen of the air, but a few better when air is excluded.
Lock-Jaw.—The bacillus of tetanus or "lock-jaw," is one of the latter class. The dust of out-buildings, the soil of gardens are favorable places for the growth of the tetanus bacillus. "Rusty" nails are common about such places. A wound is received by such a nail. The patient possibly develops lock-jaw, not because (as is popularly believed) the nail was rusty, but because, among the minute particles of dirt upon the instrument were the germs of the disease. The depths of this small wound, the superficial tissues closing and excluding the air, thus give a most favorable nidus for the growth of the tetanus bacillus.
Sunlight and Bacteria.—Sunlight antagonizes the growth of most germs. Temperature is a most important factor. The body temperature is a favorable one for many pathogenic germs, freezing, or even a temperature of 200 degrees Fahrenheit below zero, does not kill bacteria, but only arrests their growth. Favorable temperature will again restore their activity. High temperature, on the contrary, destroys them. The Jewish idea of purification by fire was based upon a scientific fact. As a practical fact boiling water kills in a few minutes most disease-producing and death-dealing germs.
Special Surgical Germs.—There are quite a known number of germs which are particularly the surgeon's enemies. Such are the following:
Pus-Producing Germs.—Pus-producing (pus being commonly called "matter") microorganisms, of which there is a large variety of cocci, must always be reckoned with. It must be understood that pus can be formed only by the presence, growth and action upon the tissues of some of this variety of germs. The formation of pus is called suppuration; the term purulent means pus-like or forming pus.
The Bacillus of Tuberculosis forms "cold" abscesses, produces "white swelling," Pott's disease, "scrofulous" conditions, besides the dread disease of consumption of the lungs. There is not a tissue of the human body which it may not ravage.
The Coccus of Erysipelas, the coccus of gonorrhea, the bacillus of tetanus, the bacillus of syphilis are common combatants of the surgeon.
|
|
|
|
|
|
|
Introduction of Microbes into the System.—A most important and practical question arises, How do disease-producing germs gain entrance into the living tissues? We daily breathe, eat and drink germs and are clothed in them. All common objects, including clothing, coming in contact with the skin, deposit bacteria upon it, so that unless rendered free from them, by special means, there is no portion of the skin upon which they do not exist. Keen says that the hands of the bride at the altar are surgically filthy.
Abundance of Germs.—Germs being plentiful in air, food and drink there is scarcely any portion of the lining or mucous membrane of the alimentary (food) canal or of the respiratory passages but what is in contact with them. Let the skin and mucous membrane be healthy and very few microbes enter the tissues; they are cast off harmlessly. But let there be inflammation or some unhealthy state of the surface, especially some "raw" spot, though ever so little, a prick, a scratch, the slightest break of skin or mucous membrane and the door is wide open for the entrance of the host.
Tissues that Assist Germs.—Providentially, certain tissue elements, notably the white blood cells and blood serum, have great capability of destroying germs which gain ingress into the system. "There is a battle royal between the invading host of germs on the one side and these defensive elements upon the other." If, for a time, the germs gain the ascendency, manufacturing their poisonous products, as they do, the subject is ill. Whenever the protective elements are conquerors the subject remains unharmed—in health. If, for any reason, a person becomes debilitated, the germ killing power of the tissue cells is less vigorous; if any portion of the body becomes injured this reduces the cell vitality at such site. The latter conditions thus render the tissues a favorable soil for germ growth.
Definition of Terms.—A germicide or disinfectant is an agent fatal to bacteria. The destruction of germs in clothing, in excrement, in a wound, on the hands, and so forth, is called disinfection. Disinfection of a wound, dressings or instruments is called sterilization. An antiseptic is an agent which retards or prevents the growth of germs. By sepsis or infection is commonly meant a condition in which disease-producing germs are present, e. g., a septic or infected wound. Asepsis means, commonly, the absence of bacteria.
Disinfection or Sterilization.—The paramount object of the surgeon in every operation to-day is to have the field of operation and all objects coming in contact with the wound as free from bacteria as may be—to do an aseptic operation. If the area of operation is already infected, for example, an abscess to be opened, he uses the antiseptic method. Three means of sterilization are available, as follows:
|
|
|
|
|
|
|
1. Thermal Disinfection consists in the use of heat in the form of boiling water, steam or hot air. By this means everything concerned in an operation may be sterilized except the skin of the patient and the operator's hands. In a modern hospital special sterilizers are used in which dressings, towels, sheets, operating gowns and so forth, are subjected to steam under high pressure. These articles, wrapped in sheets or placed in sterile jars, are not disturbed until the time of operation and are then handled with sterile hands. As a practical fact, simple boiling for fifteen minutes is a most efficient method of sterilizing, and the one which is universally used for instruments. Any clean, flat pan may be used for boiling the instruments. A teaspoonful of cooking soda to the pint of water should be added.
2. Chemical Disinfection.—Many chemicals will kill bacteria, but the most reliable and the one most common is bichloride of mercury or corrosive sublimate. (Bear in mind that it is a rank poison.) It is used in the strength of 1 part of the drug to 1,000, 2,000 or more of water. Seven and a half grains make, when added to a pint of water, a 1 to 1,000 solution. It is put up in tablets each one containing seven and a half grains. Needless to say it is not used upon mucous or serous membranes except in very weak solutions (1 to 4,000 or more). It cannot be used for the sterilization of instruments as it corrodes all metallic substances.
Carbolic Acid is valuable as a germicide in the strength of 1 to 40 or 1 to 20 parts of water. In such strength of the solution instruments are sometimes placed during operation, and it is occasionally used in cleaning the skin.
Creolin and Lysol may be used in one per cent. or two per cent. solutions upon the skin or instruments, but are chiefly employed in the former strength for vaginal and uterine douching.
Hydrogen Peroxide is an excellent agent for cleansing infected wounds. The common form should be diluted one-half or two-thirds. It is most conveniently used with an atomizer.
Normal Salt Solution, made by adding a teaspoonful of table salt to each pint of water and boiling to sterilize, is mildly antiseptic in action. It is much used for flushing out cavities of the body, e. g., the abdomen where strong antiseptics are injurious. It is often used with great advantage to cleanse large superficial wounds, such as burns or to saturate dressings applied wet. As a simple ready household remedy for cleansing wounds, gargling the throat, and so forth, it is frequently valuable.
|
|
|
|
|
|
|
Boric Acid in a saturated solution (fifteen grains to the ounce of water) is mildly antiseptic and is very commonly employed for cleansing wounds of the mouth, nose, for washing the eye in inflammations. It is a useful remedy and may be employed freely with impunity upon the most delicate tissues. In the form of powder it is frequently, with good effect, applied to cuts or other wounds.
Iodoform, in powder, is a valuable antiseptic and is much used for dusting purulent or suppurating areas. It is particularly useful in tuberculous foci. Cheese-cloth impregnated with it is largely used for draining wounds, keeping abscesses open, for packing cavities to arrest the oozing of blood.
Acetanilid, a white powder, is a fair substitute for iodoform, except that it probably does not benefit tuberculous conditions.
3. Mechanical Disinfection.—This consists practically of thorough washing with soap and warm sterile water. It will be described in detail Under the next heading.
Preparations for an Operation.—The patient should be prepared the day previous. Suggestions for such preparation are found in the chapter upon Anesthesia. A room for operation should contain as little as is essential for the necessities of the case. Some graver operations, such as those upon brain, lungs or abdominal cavity had much better be done in a hospital with all modern equipments and conveniences. However, the room of a private house may be rendered fit.
A Fit Operating-Room.—A room should be well lighted and ventilated and warm. The day before operation curtains, all hangings and carpets should be removed. The floor must be thoroughly scrubbed, the walls and ceiling brushed, or better, washed. Air, unless dust-laden, does not carry germs in sufficient numbers to infect the wound seriously. The room is to be well aired and dried. The day of operation a table (a kitchen table does well) is provided for the patient upon which are placed a folded comfortable or folded blankets. A rug or piece of carpet is spread beneath the table.
Other Preparations.—Two or three other tables or stands are placed near for instruments, basins and dressings. Buckets for the slops should be placed near. Several gallons of water thoroughly boiled must be provided. A portion should be hot, but much of it should be cooled by setting it aside in clean vessels under cover. A half dozen clean sheets and a dozen small towels should be at hand. A stove furnishes heat for boiling the pan containing instruments.
|
|
|
|
|
|
|
The Surgeon's Preparation.—The surgeon and his assistants remove their coats and roll the sleeves above the elbows. The hands and arms are to be freed so far as possible from germs—to be disinfected. A common and good method is as follows: Trim the nails short, clean well under them, removing also any excess of skin at the roots. Scrub the hands and forearms very thoroughly for five minutes or more with hot sterile water and a good soap, such as castile. A nail brush must be used; scrub very carefully about and under the nails and between the fingers. Give particular care to the creases of the hands. The nails are again cleaned with a knife and the hands afterward scrubbed. The hands are now thoroughly washed in plain sterile water and had better be dipped in alcohol for a few moments. The hands are last scrubbed for at least a minute in bichloride of mercury, 1 to 1,000, careful attention being given to the region of the nails.
The surgeon and assistants now envelop themselves in sterile gowns and scrupulously avoid touching any object which has not been sterilized.
The Assistant's Duty.—Meanwhile one assistant has sterilized the skin of the patient. The field of operation, including a wide area about the place of incision, should have been, the day before, shaved if hairy, sterilized, and meanwhile protected with sterile dressing. Whether so or not, the part, by the method used for the surgeon's hands, is disinfected immediately preceding operation. Sterile sheets and towels are now spread over the patient about the area of operation, leaving only a small portion exposed. With sterilized instruments and sponges (the latter preferably being a small strip of cheese-cloth rolled into a mass) sterilized material for tying blood-vessels and suturing the wound, the surgeon is disappointed if he does not have an aseptic wound—one that heals readily without pus formation. In such an operation chemical antiseptics, which are irritant, are avoided. If, however, a purulent condition existed prior to operation, e. g; an abscess, chemical disinfectants, notably corrosive sublimate solution, are, in addition to the former method, freely used, and the wound is probably left wide open for drainage of the pus.
Infection of Wounds.—Any wound accidentally received is infected, from the instrument wounding, from clothing, soil ground into it, in fact, anything coming in contact with it. One object of highest importance is the disinfection of such wound. For further discussion see Wounds.
Tying and Sewing Wounds.—For tying or ligating blood-vessels, silk or catgut, usually the latter, is used. For sewing or suturing a wound, catgut, silk, silk-worm gut, or silver wire are common. Catgut must be prepared by a special process. The other material is best sterilized by boiling.
|
|
|
|
|
|
|
Dressings for Wounds.—Dressings may be made of any material which readily absorbs wound fluids. Cheese-cloth is best. This, together with gowns, sheets and towels is not readily prepared without special sterilizers. In emergency, however, after boiling, drying and wrapping them in sheets or towels they may be baked. Or clean unsterilized sheets and towels may be wrung out of bichloride of mercury solution and thus, damp, be put about the site of operation. Unsterilized dressings may be treated likewise, and so placed upon the wound.
Contusions.—By a contusion or bruise is meant the crushing or laceration of tissues beneath the skin, the latter remaining unbroken. Blood is poured out into the injured tissue making it "black and blue." The effused blood will, as a rule, be gradually absorbed and the injured tissue restored. Suppuration or gangrene rarely occurs.
Symptoms.—The symptoms are swelling, tenderness, numbness, followed by aching pain. Discoloration sooner or later appears. Loss of function may occur, and, in severe contusions, shock may be great.
Treatment.—If shock is present, reaction from it should be secured by rest in bed, stimulation and external heat. Rest and elevation of the injured part are of prime importance. Application of cold is indicated, except in very grave contusions, and in the feeble and aged. Heat, instead, is indicated in such cases. Compression by firm bandage is useful for the arrest of hemorrhage and to antagonize swelling.
Accessory Treatment.—The constitutional treatment is the same as that for inflammation. Massage, liniments, applications of ichthyol ointment and motion are essential in the late stages of contusions.
Wounds.—A wound is an injury in which there is a break or division of the tissues by some sudden force. In the sense here used, the term includes tearing or dividing of the skin. Wounds comprise cuts, stabs, gun-shot wounds, bruised and torn wounds, poisoned wounds, and so forth.
Danger from Wounds.—The danger of a wound depends upon its depth and size, and above all upon the importance of the underlying parts involved, such as arteries and nerves, or vital organs, such as the heart and lungs. Stabs and gunshot wounds are generally far more dangerous than would appear from their size, because they are apt to involve vital portions of the frame, and also because pieces of the weapon or of the bullet may be left remaining in the wound, as was the case with the lamented President Garfield.
|
|
|
|
|
|
|
Healing of Wounds.—The healing of wounds occurs in two ways:
By First Intention.—In the first place, a wound may heal by primary union, or, as it is also called, union by the first intention, without the formation of any pus or matter, and leaving only a very fine line-like scar. This mode of healing should always be sought for, but can seldom be obtained, except under the following conditions, to wit: when the sides of the wound can be accurately fitted together, and are not subsequently displaced by bleeding or the exudation of matter, also when the wound is left quiet and protected from outward injury, and when it is kept free from impurity.
Healing by Second Intention.—The second mode of healing takes place slowly, with suppuration and the formation of little rounded knobs, called granulations, all over the raw surface, and leaves a large, red scar, ultimately becoming dead white. This second and far inferior method of healing is observed when the favorable conditions just mentioned are absent, as for example, first, when so much of the skin has been destroyed that the edges of a wound cannot be brought together, as in wounds caused by cannon balls or shells, in scalp wounds from blunt instruments, or where the edges of wounds are so torn and bruised that their life is crushed out; second, where the edges of wounds are separated after they were adjusted, by blood being effused, or by the formation of pus; third, when the injured parts have been disturbed, as, for instance, in the leg, by standing or walking, or the hand and arm by working, and so forth; or, if the wounded party has been badly transported from the scene of the accident; or, lastly, when the wound was dirty and had not been properly cleansed or disinfected, because want of cleanliness leads directly to putrefaction and the formation of pus, and it is especially the matter formed in the process of suppuration which separates the sides of wounds and prevents their healing by the first intention.
Proud Flesh.—When the wound does begin to heal in the second and inferior method, granulations form, which are often called proud flesh, and are especially dreaded by ignorant persons as dangerous intruders into a sore. These granulations by degrees organize into a living tissue of great, firmness, and after they have filled up the cavity of the wound to the level of the surrounding cutaneous surface, or sometimes a little above it, they cover themselves with epidermis and constitute a scar.
Symptoms.—The symptoms of a wound are constitutional and local. The constitutional or general effect of a serious wound is called shock. In shock, sudden depression of the vital powers occurs. There is general
(Continued on page pg0657)
|
|
|
|
|
|
|
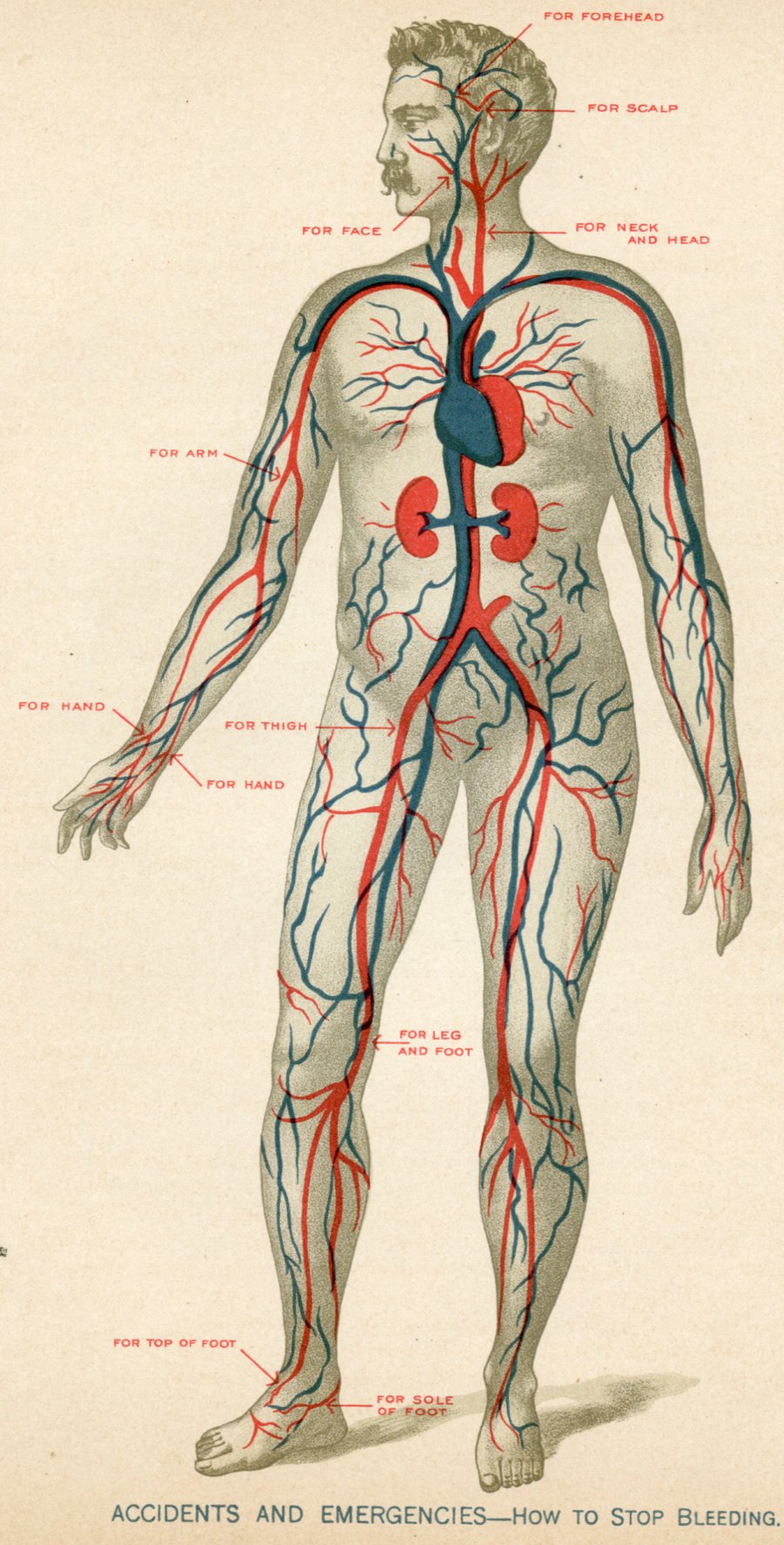
The Emergency.—In case of severely bleeding wounds, quick work is required to save life. One must know not only what to do, but how to do it.
The Arrows.—The arrows in the adjoining plate show the places on the body where pressure is to be made in order to stop the flow of blood.
Kinds of Pressure.—In ordinary wounds the pressure may be found sufficient when made with the index finger or the thumb. In severe wounds, and where the arteries or veins lie deep, the firm pressure of both thumbs may be required. And where the wounds are still more severe, or pressure with the thumbs becomes tiresome, resort may be had to a large key, or better still, to the familiar and effective appliance known as the Spanish windlass, or to the tourniquet made of a strap; cord or handkerchief. For a full description of "How to Arrest Bleeding" by exerting pressure, see pages 656-668.
Places of Pressure.—1. If the wound is upon the forehead, place the index finger or thumb upon the spot indicated by the head of the "forehead" arrow, and exert firm pressure.
2. If the wound is upon the scalp, place the index finger or thumb upon the spot indicated by the head of the "scalp" arrow, and press firmly.
3. If the wound be upon the face, place the index finger or thumb upon the spot indicated by the head of the "face" arrow, and make firm pressure.
4. If the wound be upon the head or upper part of the neck, in other words, above the shoulders, the pressure must be made on the spot indicated by the head of the "neck and head" arrow. Press hard and constantly.
5. If the wound be on the arm, make the pressure on the inside of the arm, at the spot indicated by the head of the "arm" arrow. This pressure will stop the bleeding of a wound anywhere below the neck and above the heart, but it must be made on the inside of the arm nearest the wound.
6. If the wound be on the hand, make the pressure on the places indicated by the heads of the "hand" arrows.
7. If the wound be on the body anywhere below the region of the heart, the pressure must be exerted very firmly (see page 661) on the inside of the thigh, at the point indicated by the head of the "thigh" arrow.
8. If the wound be on the lower leg or foot, the pressure must be made on the spot indicated by the head of the "leg and foot" arrow.
9. If the wound be on the top of the foot, make the pressure at the spot indicated by the head of the "top of foot" arrow.
10. If the wound be on the sole of the foot, make the pressure on the spot indicated by the head of the "sole of foot" arrow.
|
|
|
|
|
|
|
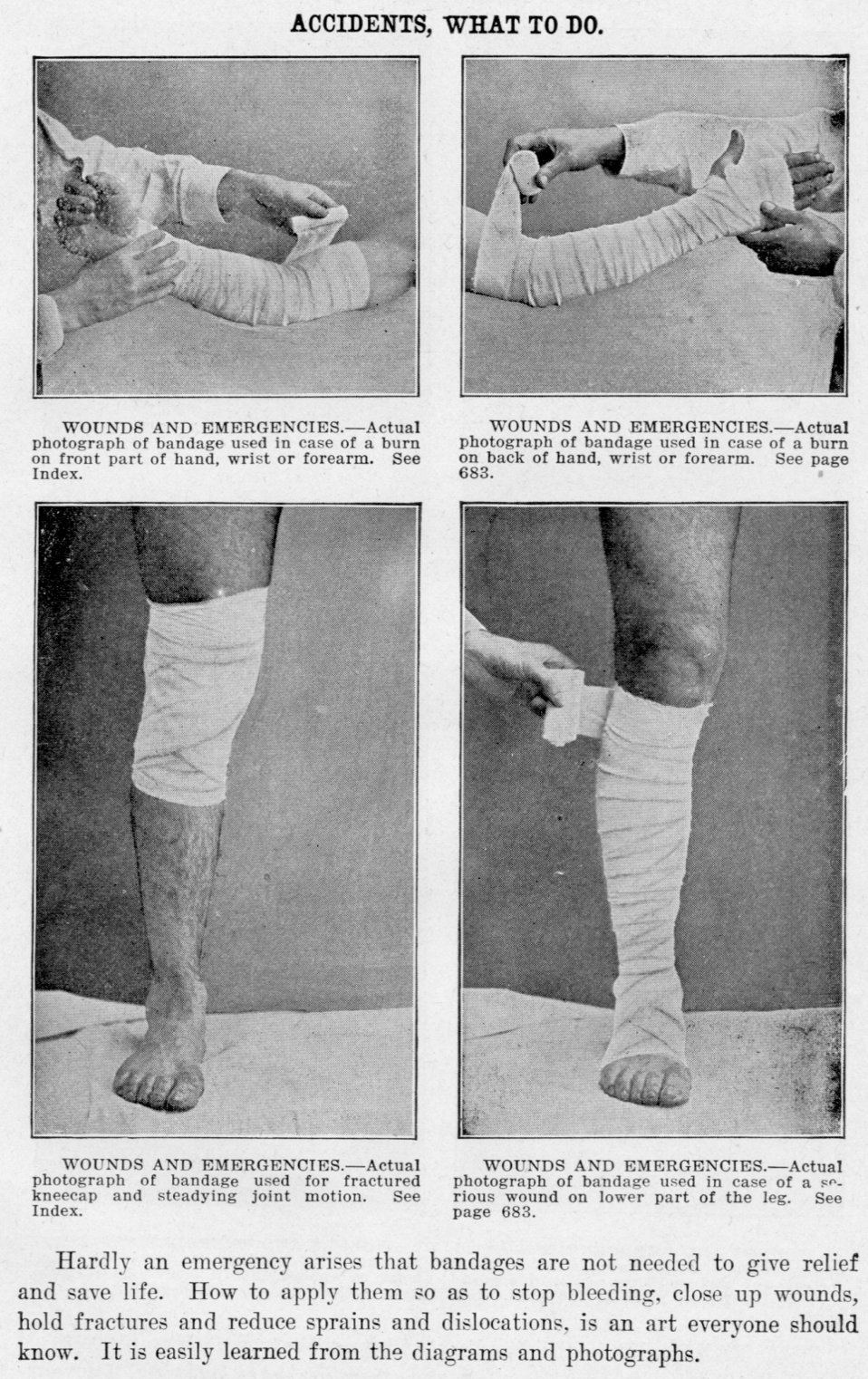
Hardly an emergency arises that bandages are not needed to give relief and save life. How to apply them so as to stop bleeding, close up wounds, hold fractures and reduce sprains and dislocations, is an art everyone should know. It is easily learned from the diagrams and photographs.
|
|
|
|
|
|
|
THE BANDAGE is the handiest and mightiest of factors in cases of accidents and emergencies. Its quick and ready use saves suffering, deformity and life itself. The diagrams and photographs explain the manner of applying bandages to meet emergencies.
|
|
|
|
|
|
|
weakness; a faintness, with sometimes loss of consciousness; the pulse is feeble and rapid; skin pale, cold and clammy; the bodily temperature is lowered; nausea with vomiting may occur. Loss of blood may be a strong factor in producing shock.
Reaction from Shock.—During and following the arrest of hemorrhage, reaction from shock is to be sought by raising the feet and lowering the head; at least place the head flat, and the lower extremities quite as high as the head; wrap the patient in warm blankets and surround him with hot bottles, hot bricks, and so forth.
Stimulants.—A tablespoonful of whiskey or brandy may be given by mouth every half hour. An enema of black coffee one-quarter pint and whiskey two tablespoonfuls is excellent. Injections under the skin of whiskey, strychnine, digitalis, are invaluable. In the graver forms the injection of large quantities of warm normal salt solution beneath the skin, into the bowel or into the veins should be practiced.
Local Symptoms.—These are hemorrhage, pain, loss of function and gaping of the wound edges.
Treatment of Wounds.—The steps in treatment of a severe wound are given in order as follows:
Arrest of Hemorrhage.—The fact that hemorrhage may readily prove fatal, or, as it is popularly phrased, the person may easily bleed to death, is so important that a detailed discussion is needful. Every wound bleeds, because in every wound blood-vessels are injured. But the kind of hemorrhage, as well as its danger, varies with the size and the nature of the blood-vessels which have been divided. If the blood does not flow freely, but trickles from the wound, one may conclude that only small blood-vessels have been severed. When dark blood wells out in a steady stream, and when the flow is increased by pressure above the injured spot, that is, nearer the heart of the patient, a large vein has been opened. Lastly, when bright, red jets spurt out of the wound, forcibly, and in jerks, an artery is divided and danger to life is great and immediate.
Smaller Wounds.—Unimportant hemorrhages from very minute arteries, and from veins of only moderate size, can generally be arrested by pressure upon the wound itself, or by pressing the sides of the cut against each other, or it may stop of its own accord in consequence of the mouths of the vessels contracting and the blood in the wound coagulating into a tough, viscid mass.
Hemorrhage from an injured vein, as, for example, that from the giving way of a varicose vein in the leg, is sometimes difficult to check, on account of the pressure of some light article of clothing, such as a garter,
|
|
|
|
|
|
|

What to Do.—This class of common and dangerous emergencies may be successfully met on the moment by the simple means shown, in the adjoining plate. By preventing the poison from entering the system, time is gained for the use of the remedies given on pages 365, 664, 1034.
The Band.—The band, fillet or ligature used may be a strap, cord, rope or handkerchief—anything, in fact, which can be drawn and tied tightly; or which, if tied loosely, will permit of a stick being placed within it, and a tight twisting of the same, after the manner of a tourniquet (see page 660), in order to stop the blood circulation more effectively.
How to Do.—1. If the bite be on the arm, bind the cord, or ligature, tightly around the limb at the point indicated by the head of the "arm" arrow.
2. If the bite be on the hand, bind the cord tightly around the wrist at the point indicated by the head of the "hand" arrow.
3. If the bite be on the upper part of the leg, bind the cord tightly around the limb at the point indicated, by the head of the "upper limb" arrow.
4. If the bite be below the knee, bind the cord tightly around the limb at the point indicated by the head of the "lower limb" arrow.
5. Further Precautions.—It is perhaps unnecessary to add that in the emergency of a mad dog bite the band for preventing the virus from entering the system should be applied as quickly and tightly as possible. If the material is at hand, several of such bands, tied one above the other, will prove more effective than a single one. An additional emergency measure, and a very proper one, is to quickly cut the wound out with a sharp knife, and then to cauterize it with a hot iron, or such other means as may prove to be at hand. Make all haste to get the victim within reach of the remedies given in the pages above mentioned.
The Snake Bite.—The snake bites that are dangerously poisonous are those of the copperhead, water-moccasin, rattlesnake and viper. As in the case of the mad dog bite, several bands, tied one above the other, are better than one. The wound should be cut out, and then sucked. No harm can come from this if the mouth be free from sores, or the poison is not swallowed. In the absence of other means of cauterizing a snake bite wound, hunters pour powder upon it and explode it with a spark. The band or bands used should not be removed for some time, and in case of more than one, the uppermost one should be removed first, above the bleeding point. On loosening this, slight pressure upon the wound and elevation of the foot above the level of the hip suffice to arrest the bleeding.
|
|
|
|
|
|
|
Control of Hemorrhage by Compression.—If, however, bright, red blood continues to flow, in spite of pressure over the wound, a large artery must have been injured, and speedy death from loss of blood must be apprehended. In such instances, prompt aid is necessary, and a physician or surgeon should at once be sent for.
Where to Place Pressure.—Until he arrives any intelligent person can probably succeed in checking the flow of blood by making very firm pressure on the wound itself, if it is small, or on the trunk of the artery above the wound. The injured limb should be raised, as this lessens the force of the pulse in it, and, of course, the violence of the flow of blood. After cutting the clothing away from the source of hemorrhage, a folded piece of clean linen, or a pocket-handkerchief, should be laid on the wound, and fastened firmly down by means of a bandage or another handkerchief. But if, in spite of this, the blood still continues to run, the trunk of the artery between the heart and the wound must be sought for and firmly compressed by the fingers, the handle of a large key, or some ether suitable object. In certain parts of the body the arteries lie so near the surface that they can be effectually compressed with the fingers.
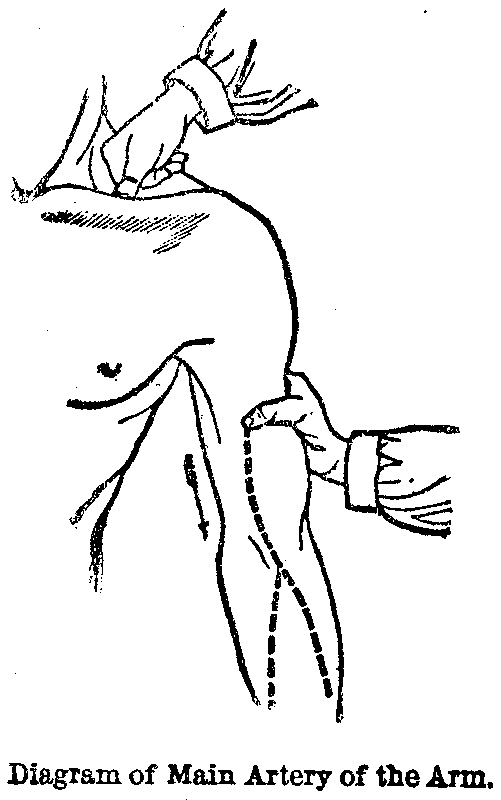
Pressure on Arm Artery.—In the upper part of the arm the main artery courses along the inner side, nearly in a line with the inner seam of the coat or dress sleeve, as is shown in the accompanying figure. By feeling along the place indicated by the dotted line, it is easy in any spare person to discover the strong pulsation of this large artery of the arm, or brachial artery, as it is technically called. The artery may be compressed in this position by placing a thick stick between the arm and the chest, and tying the arm tightly to the body, or by pressing the artery firmly against the bone of the arm with the thumb, as shown in the illustration.
Pressure at Collar Bone.—Sometimes, when the wound is higher up on the arm, or in the arm-pit itself, it may be necessary to compress the artery at a point nearer the heart; and this can usually be accomplished by making pressure with the thumb or a big key, Just behind the collarbone, as is also indicated.
|
|
|
|
|
|
|

The Spanish Windlass.—If it is found difficult to continue the application of force in these situations, or if the only person present must leave the sufferer whilst he hurries off for assistance, the little device known by the name of the Spanish windlass should be resorted to. To apply this, take a large handkerchief and fold in it a rounded pebble about an inch in diameter, or any other smooth, hard body of similar size; fold the handkerchief cravat-shape, and tie it loosely about the limb, at the point where pressure is to be made upon the artery; and then, putting a stout stick beneath the loop, twist it around so as to tighten the handkerchief and bring a strong pressure upon the stone underneath the loop on the side opposite to the stick, which in its turn compresses the artery and stops the flow of blood. This is, of course, a much more painful, as it is a more powerful method than pressure by a bystander's thumb or finger; but in urgent cases it may be needful to call it into service in order to save life.
The Tourniquet.—The Spanish windlass is a rough imitation of the surgical instrument called a tourniquet, which is far preferable as a means of arresting hemorrhage whenever it can be procured. As soon as a tourniquet can be obtained, it should be substituted for the primitive and painful windlass, which, if continued several hours upon a limb, might itself lead to mortification of the part, and perhaps to a fatal result.
Treatment With a Handkerchief.—In order to check bleeding from wounds in the arm below the elbow, or about the hand, where workmen of all kinds are particularly apt to receive injuries, take a large handkerchief, as before, and tie up in it a stone or a potato of the size of a walnut, or a simple, large, hard knot will perhaps answer the purpose. Then fasten it loosely about the arm, just above the elbow, as shown in the illustration, and bend up the forearm so as to make the knot press upon the large artery in its position in the hollow of the elbow, as indicated in the accompanying wood-cut. If the hemorrhage is found to be checked, the knot is in the right place at the bend of the elbow; but if blood continues to flow, straighten the arm, move the knot or stone a little, and try it again. As soon as you find the flow of the blood is stopped, take another large handkerchief, or a strip of bandage, and fasten the wrist firmly to the shoulder, so as to keep up the life-saving pressure upon the blood-vessel at the elbow.
|
|
|
|
|
|
|

Wounds Below the Knee.—Hemorrhage from wounds of the leg, below the knee, or of the foot, such as are so often inflicted by the slipping of an axe or hatchet in chopping wood, may be controlled in a very similar way by tying a large pebble in a handkerchief, so as to make a knot the size of a turkey's egg, fitting it in the hollow of the knee, and then bending the leg up on the thigh in such a manner as to produce pressure upon the artery, on exactly the same principle as that displayed in the figure just above. When it is found that the knot is properly adjusted, so as to answer the purpose of arresting the flow of blood, the leg should be secured in its doubled-up position in order to prevent a return of the hemorrhage, in consequence of the apparatus becoming displaced.
Thigh Wounds.—For bleeding from wounds in the thigh, the artery must be compressed an inch or two below the middle of the groin, and about as far in front of the usual position of the inner seam of the pantaloons. The exact point is indicated by the marginal illustration, which shows very well the way in which the thumbs ought to be applied.
Pressure on Thigh Artery.—The femoral artery, or artery of the thigh, is so large and strong that its pulsation can usually be felt without much difficulty in thin or even moderately spare persons; and it is a good plan for every one to become acquainted, by examining his own body, with the location of this and the other chief arteries. This point in the femoral artery is also a favorable one for making compression in bleeding wounds of the foot and leg.
Fainting Fit.—In whichever way bleeding from an important artery has been for the time checked, it must be remembered that it is very liable to burst out again the moment the pressure is relapsed or the obstruction removed; also, that when a person faints from loss of blood the hemorrhage ceases whilst the heart is beating feebly in the fainting condition, and the blood may clot quite firmly in the mouths of the divided blood-vessels. When, however, the patient revives the renewed vigor of pulsation in the heart and arteries will generally drive out these recently-formed clots of blood, and the bleeding starts afresh with, perhaps, a speedily fatal result, if a most vigilant watch is not maintained over the wound. Where the hemorrhage is venous only, however, there is a good prospect that tue clots of blood formed in the open mouths of the vessels will be able to resist the feebler pressure brought to bear upon them by the reviving circulation, and that bleeding will be effectually checked by the occurrence of the fainting fit.
|
|
|
|
|
|
|
Tying of Blood-Vessels.—In order to obtain primary union, it is necessary, in dressing a wound, to stop all hemorrhage. A surgeon grasps with forceps the end of any vessel that bleeds considerably, and before closing the wound ligates or ties it. Sterilized catgut is best for ligatures, but silk, or even cotton thread that has been boiled, will answer. Simple twisting with forceps will arrest hemorrhage of very small vessels, while oozing is generally controlled by pressure with compresses wrung out of water as hot as can be borne by the hand.
Reaction from Shock.—See Shock.
Cleansing of the Wound.—This includes the removal of both foreign matter visible to the eye, and the removal as well of microscopic germs which contaminate every accidental wound. Have at hand plenty of water and good soap. Scrub the wound and surrounding area thoroughly with soap, with scissors and forceps removing any visible foreign matter (splinters, bits of clothing, grains of dust or hopelessly damaged tissue). Wash with plain water and alcohol and irrigate with corrosive sublimate solution (1 to 1000). If the wound is of a hairy part, the area should be shaved. All blood clots should be removed and the wound left clean and dry.
Provision for Drainage.—Most accidental wounds, unless small and superficial, should be left partially open for drainage, so that infective material which it has not been possible to remove, may flow out. In such cases, a bit of rubber tubing may extend to the depth of the wound or a strip of iodoform gauze, or plain sterile gauze may be gently inserted to the depth of the wound, one end of the strip protruding. A few strands of suture material well serves the purpose.
Closing of the Wound.—Where confidence of thorough disinfection is felt, and the loss of tissue is not too great, the edges of the wound should be brought together and the tissues held in the relation they bore before injury. Sewing or suturing a wound is the best means to this end. Surgeons use special needles and a variety of suture materials, silk, silver, wire, silk-worm gut and specially prepared catgut. In an emergency, however, a large sewing needle and large-sized cotton sewing thread, which have been boiled, may do good service. Interrupted stitches (each stitch tied separately) are usually the better. The edges of a superficial wound may be held together by strips of adhesive plaster placed outside of the dressing of the wound. Or, in slight cuts and abrasions, collodion painted over a bit of dressing is sometimes efficient.
|
|
|
|
|
|
|
Dressing of the Wound.—Any aseptic or antiseptic material which absorbs wound discharges freely, such as absorbent cotton, cheese-cloth or even thin old muslin forms a good dressing. Sprinkling the wound freely with an antiseptic powder helps to prevent suppuration; dressings had better be applied moist, wrung out of bichloride of mercury solution (1 to 2000). Plentiful dressings should be applied, sufficient to soak up the wound discharges and to protect from outside infection. A wound should be disturbed for dressing as seldom as possible. If the dressings become soaked with wound fluid, if there is much pain, or a rise of temperature indicates suppuration, the wound should be freshly dressed; otherwise, the dressing should remain in place a week or ten days.
Securing Rest.—In case of severe wounds, not only should the patient rest in bed but absolute rest to the part should be secured. Compression by firm bandage, an easy relaxed position, fixation by splint or plaster dressing, support of the arm in a sling, these all give comfort and hasten healing of a wound.
Constitutional Treatment.—General treatment should be according to the suggestions for the treatment of inflammation; in addition, watch for suppuration, gangrene, erysipelas or tetanus. Temperature is a good index of the condition.
Punctured Wounds.—Wounds made by sharp instruments (such as a dagger, a splinter, a fork prong, and so forth) have especial dangers, and require radical treatment. Foreign bodies are frequently left at the depth of such a narrow wound; the opening is small and readily closes, locking up infective material; underlying organs of the abdomen, head or chest are liable to injury. Such wounds generally demand the attention of the skilled surgeon. He will usually probe for a foreign body and will generally open the wound to its depth, often incising it freely, in order to disinfect it properly and to allow for drainage. He will determine whether underlying organs are injured and any treatment needed for such.
Gun-shot Wounds.—The special dangers to be combated in gun-shot wounds are shock, hemorrhage and infection. Injury of vital organs is liable. In many cases it is better not to probe for a bullet. The ball should be searched for when it has surely carried in with it foreign bodies; when it is in a vital organ, as the brain; and when its presence interferes with healing.
|
|
|
|
|
|
|
Poisoned Wounds.—Dissection wound is a term applied not only to wounds received by medical students and surgeons in their dissections, but to wounds sometimes received by butchers, cooks and fish-dealers, who handle putrefying animal matter. Such wounds are particularly virulent. A wound of this character should be thoroughly washed, and the blood squeezed out of it. If a puncture, it should be freely opened and swabbed with pure carbolic acid, then washed with bichloride of mercury solution, and wet antiseptic dressing applied. Bites by animals should be so treated, the human bite being one of the worst.
Stings and Bites of Insects.—For the more common and less poisonous wounds, applications of solutions of washing or cooking sode[sic], ammonia water, iodine or lead-water and laudanum, give relief. The bite of a large spider or scorpion should be treated as a snake bite.
Snake Bites.—Copperheads, water-moccasins, rattlesnakes and vipers are the only poisonous snakes of the United States. We have a poisonous lizard known as the "Gila monster." A snake bite must be treated promptly and usually without proper appliances. When the bite is upon a limb, very tightly tie or twist a band or fillet around the extremity above the wound; several such bands are better. Cut out the wound at once, suck the wound, burn it with nitric or carbolic acid or heat. A hot iron is efficient; hunters may pour powder into the wound and apply a spark or lay a live coal upon it. Constitutionally stimulate freely with whiskey or brandy to sustain the system while it is ridding itself of the poison. Strychnine, ether and digitalis hypodermically are valuable. The fillets should not be removed for some time, and then slowly, one at a time, the uppermost one first.
Hydrophobia or Rabies.—This is an infectious disease due to inoculation through a wound with the virus from a rabid animal. The animal may be a dog, a cat, a wolf, a fox or a horse. About 14 per cent. of the people bitten by mad animals develop the disease and die.
Treatment of Hydrophobia.—When a person is bitten by a supposed rabid animal and is seen soon after the injury, firm constriction of the part above the wound should be made, the wounded area should be freely cut out, burned with a hot iron or nitric acid and dressed with wet antiseptic dressing. If the patient is not seen within a few hours of the injury, cauterization will do no good. In any case, send the patient to a Pasteur Institute for preventive treatment. If the animal causing the wound was not rabid, treatment will do no harm; if it was mad, treatment will probably save the patient.
|
|
|
|
|
|
|
Careful Handling.—In moving a wounded person from the scene of accident, the chances of recovery are often very much increased by adopting the method involving the least amount of additional injury to parts which have already suffered. The dangers to life from a broken leg, for example, when the skin is not cut through, are more than doubled, if, by ignorant handling, with the kindest intentions in the world, the affected limb is allowed to swing downward for a single instant so that some sharp splinter of bone penetrates the skin, and makes the injury a compound fracture.
An Improvised Stretcher.—The best method of moving a person who is unable to walk, is upon a stretcher or litter, which may be a light lounge or bedstead, an old-fashioned settee, a long bench, a door or window-shutter slipped off its hinges, or a simple, broad board. Such hard materials should be covered with blankets, quilts or the coats, and so forth, of bystanders. In the woods, two poles about ten feet long, kept apart by forked sticks about a foot in length, tied in place with rope, twine or leather straps, or even some climbing plant, and covered with clothing, form a very good litter.
Loading the Stretcher.—To place the helpless patent[sic] upon such a vehicle of transportation, the litter should be set down with its foot at the head of the patient as he lies upon the ground, and in a line with his body. Then, if there is plenty of assistance at hand, let the acting surgeon of the party take charge of the wounded limb, and devote himself, after giving the necessary instructions to an acting assistant surgeon chosen on the instant, to protecting that injured member in every way. Next, let four persons, under direction of the assistant surgeon, lift the sufferer by his hips and shoulders, two others supporting the head and feet, as may be necessary, and when raised to a sufficient height, let two others, still, slide the prepared litter under the patient as he is held up in the air by his seven bearers. He can then be gently deposited upon the litter, having undergone the least amount of disturbance possible under the circumstances.
When Only Two Persons are Present.—When but few persons are present, this plan of procedure, must, of course, be modified; and if the services of only two people are available, it is better, usually, for them to lift the wounded man together, both standing on the same side, one at the shoulders and the other near the hips, and tenderly lay him upon the litter, which has been placed at the opposite side.
|
|
|
|
|
|
|
Other Ways of Handling Wounded.—Another mode, which, answers very well when the lower limbs are not injured, is for the two bearers to stand on opposite sides of the patient, and, clasping each others hands beneath his hips and shoulders, carry him a few steps to the litter, which has been arranged with its foot to his head, as directed above, in the first instance. If alone with an individual so severely wounded as to be helpless, the best way often is to make him as comfortable as possible, see that there is no danger of serious bleeding, leave him some weapon with which to defend himself, and hasten for the nearest assistance which can be procured.
Carrying the Litter.—The litter should be carried by two persons, whilst the acting surgeon walks by the side and keeps a constant watch over the patient. The following rules should be observed: First, the litter should be carried with the hands, or supported by straps passing over the bearers' shoulders. The litter itself should never be placed upon the shoulders of the bearers, because the patient might then fall off, or even die from hemorrhage or other cause without his danger being observed.
Bearers Not to Keep Step.—Second, the bearers should not keep step. If they keep pace, as in marching, the litter shakes from side to side, and the patient is apt to roll about, or even to be thrown to the ground. To prevent this, the bearers must walk in broken step —that is, not putting the right foot, for example, forward at the same moment—and then the litter remains nearly even as it is borne along.
Pace of the Bearers.—Third, the pace of the bearers should be short, not more than twenty inches, and the steps made without any spring on lifting the foot from the ground. All jolting, all hurried movements and lifting over fences, ditches, and so forth, are to be avoided. Send some one ahead, if practicable, to look out for gates, bridges, and similar advantages, which are very important in the transportation of the sick and wounded, and let him come back and guide the bearers in the easiest path to the place of destination.
Bearers of Same Height.—Fourth, if it can be done, choose bearers of the same height, and should it be impracticable to do this, arrange the shoulder-straps in such a way that the litter will hang as level as possible. Fifth, in ascending an inclination, such as hill or staircase, the patient's head must be in front, and in descending it should be behind. If, however, the invalid has a broken leg, this rule must be reversed: otherwise the weight of the body would press upon the injured part, and, perhaps, aggravate the trouble. Sixth, the patient should usually be removed from the litter in the same manner as he was placed upon it.
|
|
|
|
|
|
|
In Absence of a Litter.—Should neither a litter nor material out of which one can be made present itself on careful search, the wounded man must be supported in the arms, which of course can only be done as a general thing for short distances. If there is only one person at hand to help, and if the injured man can walk, though weak and faint from loss of blood, he must put one arm around the neck of the individual aiding him so that his hand hangs down over the further shoulder. The person assisting places his arm from behind around the waist of the wounded man, and with his other hand grasps that of the patient as it hangs over his shoulder. In this mode he can support him very efficiently, and if necessary even raise him from the ground for a few steps over difficult places, and so help him along. Should the patient, however, be unable to walk, the only resource is for the person helping him either to take him on his back, or, if not too heavy, to carry him in his arms like a child. In either case the wounded person should clasp his arms around the neck of the bearer.
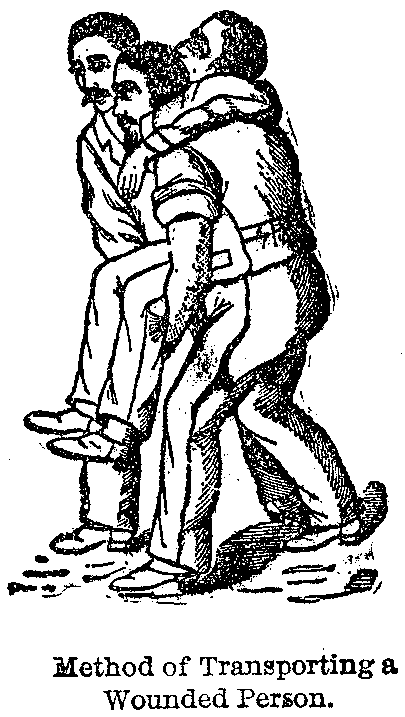
Joining Hands for a Seat.—Should there be two people at hand to render assistance, one of the best modes is for the bearers to join hands so as to form a seat, in what is popularly called among children "Lady of London fashion," and placing the patient upon this, as shows in the above picture, he may be transported for long distances with considerable ease. Should the patient be unconscious it will be necessary for one of the bearers to support the upper part of the body by walking behind him with his hands clasped upon the patient's chest, after they have been passed beneath the sick man's arms. The other bearer walking in front carries the legs of the sufferer, one under each arm.
Bed for Accident Patient.—The preparation of the bed for a patient who is the subject of a severe accident is a matter of no little importance. The couch intended for the reception of an accident case, wounded about the legs or hips, should be provided with a large sheet of water-proof material and an extra sheet folded and placed across the bed, so that it can be readily removed when soiled with blood or other discharges without disturbing the head and shoulders of the patient. If the mattress is likely to yield to any extent with the weight placed upon it, it should be supported with extra slats. In case of wounds about the head, the pillow ought to be protected by a piece of extra sheeting.
|
|
|
|
|
|
|
Undressing the Patient.—A patient who is not too much injured to endure the effort should always be undressed before being placed in the bed. All tight clothing about the neck should at once be loosened or altogether removed. Boots must be taken off with great care.
Case of Broken Leg.—If the leg is broken it is better to cut the boot down the side and nearly to the toe. Pantaloons need not be cut, unless the patient's leg or thigh is injured, in which case the outside seam ought to be ripped up, so as to get them off without causing suffering to the invalid. In taking off the coat and waistcoat always remove them from the sound side first, and then they come away from that which is injured with comparatively little difficulty.
Unloading the Litter.—When a patient who is unable to walk is brought in on a litter or stretcher of any kind, such as a window-shutter or door, the litter should be placed with its head at the foot of the bed which the invalid is to occupy, and lying in the same direction, this position being the most convenient one for transferring the sick man to his couch. To properly lift an adult patient four assistants are required, two standing on either side. One of these helpers should support the head and shoulders, and a second the hips on one side, whilst on the other side the third assistant lifts the back, and the fourth supports the legs. In some cases the size or arrangement of the room will not permit this.
Placing the Patient Abed.—The litter must then be laid alongside of the bed, and three assistants lifting the patient into the air, a fourth rapidly withdraws the litter to allow the bearers to approach the side of the bed and deposit the invalid upon it. All the assistants should commence to lift together, and set down the patient at a given signal, special attention being devoted to the injured limb. The bed-clothes should be folded back for the whole length of the bed on one side, leaving one-half of the bed laterally uncovered for the reception of the patient. By this little maneuver they are easily replaced over a frame of wire, or of two half hoops tied together in their centres, in such a way as to protect the wounded limb from the weight of the bed covering.
Definition.—Inflammation is defined as "the changes which occur in living tissue when it is injured, provided that the injury is not of such a degree as at once to destroy its life." Inflammation may end in return of the tissues to complete or partial health, or in their death. Death of inflamed tissue may occur by suppuration, ulceration or gangrene.
|
|
|
|
|
|
|
Causes of Inflammation.—The causes of inflammation are predisposing and exciting. Predisposing causes are such as are present in the tissues and render them liable to inflame; any affection or indulgence which impairs the health or weakens the system is a strong predisposing cause. Exciting causes are injuries, for example, blows, falls, crushes, burns, and so forth.
Symptoms of Acute Inflammation.—Symptoms are general or constitutional and local. The former are manifested chiefly as fever. The latter in an organ or a part, as heat, swelling, pain, discoloration and disordered action or function. Constitutional symptoms of acute inflammation may be absent, but in severe cases they are sure to occur, forming the symptom group known as fever— symptomatic or inflammatory fever.
Chronic Inflammation.—This condition is gradual in onset and progress. There are no constitutional symptoms due directly to the inflammation. As to local symptoms, there is pain, varying in degree and character; swelling is often great; function is more or less interfered with; heat and discoloration are rare.
Treatment of Acute Inflammation.—The prime rule of treatment is, first to remove the exciting cause. If it be a splinter, pull it out; if drink or indigestible food is inflaming the stomach, stop it; scrape out diseased bone, clean out the germs from an infected wound. Further treatment should be both local and constitutional.
Local Treatment of Inflammation.—Two agents are suited to the treatment of both the early and the late stages of an inflammation, namely, elevation and rest. Elevation combats engorgement of the part. A sprained ankle is more comfortable if put on a level equal with or higher than the body. Rest is of utmost importance. Rest of the patient in bed should be insisted upon in every severe inflammation. Rest to an inflamed part is secured by various means. The partial, or better, the complete cessation of the usual action or function of an organ, is desirable. To an inflamed eye, rest is secured by dark glasses, a darkened room, or a pad to exclude the light; to a sprained joint, by an easy position and fixing it on a splint, or hanging the arm in a sling.
Other Treatments.—In the early stage of an inflammation, when the vessels are engorged, local bleeding and cold are valuable agents. Local blood-letting is done by cutting, leeching or cupping. Neither of these should be done except under the intelligent guidance of a physician.
Cold is highly valuable if used wisely; it is not to be used after the early stages, not to be too long continued or too intense; it should usually not be used with the very aged or very feeble.
|
|
|
|
|
|
|
Wet cold or dry cold may be employed. Wet cold is obtained by various fluids; ice water or water mixed with one-fourth the quantity of alcohol is good. One of the most common and best applications is lead water and laudanum. It is composed of one ounce of laudanum, one or two ounces of Goulard's extract, and one part of water. A few layers of muslin or cheese-cloth should be kept upon the part and should be frequently wet with the fluid.
Dry cold is generally safer, more easily applied, more comfortable. Cracked ice is put into a rubber ice-bag or bladder, or wrapped in a piece of flannel, and so applied, several folds of flannel first being placed over the part. The immediate application of an ice-bag to a sprained joint is excellent treatment. In all applications of cold the part must be carefully watched to guard against too great interference with the circulation.
Treatment in Later Stages.—Treatment in the later stages of an inflammation is directed toward promoting a reabsorption of the material which has been poured out, a clearing up of the wreckage. This is accomplished by compression, the application of astringents and sorbefacients, massage and heat.
Compression.—Compression is usually obtained by the firm application of a bandage. It should never be forcible, and if applied to a limb, should always include the distal extremity, e. g., the elbow or wrist should not be firmly bandaged without including the hand and all the part below the affected area.
Astringents and Sorbefacients.—Lead water and laudanum, before mentioned, has an astringent effect. Tincture of iodine diluted with from one to three parts of alcohol, painted from time to time over an inflamed area, is often useful. Ichthyol ointment is very excellent in inflammatory swellings. It is rubbed well into the part or applied upon a cloth. It is best prepared by mixing one part of ichthyol with one to three parts of lanolin. Mercurial or blue ointment is used in much the same way as is ichthyol ointment.
Massage.—Massage is a systematic rubbing and manipulation after the acute symptoms have subsided. Motion and massage prevent stiffness, promote circulation and absorption, and bring tone and health to a part.
Heat.—Heat, either moist or dry, may do good and should generally be substituted for cold after a day or two. It then commonly gives greater comfort, relieving pain. Heat may be applied by fomentations, poultices, water bath or douche, and dry heat.
|
|
|
|
|
|
|
Fomentation.—Fomentation is the application to the skin of a piece of flannel wrung out of a hot liquid, usually water, as hot as can be borne. It is covered by a rubber-dam, oiled silk, or waxed paper; cotton should be placed outside the latter and the whole held in place by a bandage. A hot water bag placed over the bandage is useful.
Stupes.—The turpentine stupe is made as above by sprinkling upon the wet flannel from ten to twenty drops of turpentine.
Poultices.—A poultice is a soft mass applied to a part to bring heat and moisture to bear upon it. Poultices may be of flaxseed, arrowroot, starch, bread and milk, and so forth. A poultice should be applied in thickness of half an inch, should be covered with rubber-dam, waxed paper or oiled silk and overlaid by a hot water bag. It should be removed before it cools, another being ready to apply at once. Where suppuration is threatened or exists time is often wasted and suffering prolonged by continued poulticing. This great blunder is common with the laity. In such a case, free opening by incision cannot be done too quickly.
Dry Heat.—Dry heat can be easily applied with the hot water bag, a bag of hot sand or meal, a hot plate or bottle.
Counter-Irritation.—By counter-irritation we mean the use of some irritant upon a surface, thus attracting an increased quantity of blood and relieving thereby inflammation of a deeper structure. Blisters, mustard plasters, turpentine stupes, tincture of iodine, liniments, and so forth, are so used.
Constitutional Treatment.—General treatment may include general bleeding, circulatory sedatives, diaphoretics, diuretics, anodynes, antipyretics, stimulants and tonics. Hygienic measures are invariably demanded, cathartics are usually indicated.
Cathartics.—One of the first essentials in beginning inflammation, is free movement of the bowels. If this has not occurred spontaneously, one of several purgatives may be given. Calomel is often invaluable. It may be given in doses of one-tenth to one-fourth of a grain, repeated every hour until a grain or more is taken, or be given in one large dose of one to three grains. It may have to be followed by castor oil or epsom or rochelle salt. Either of the latter is sometimes excellent alone, a teaspoonful of each or of both being given every hour until a movement occurs. A bowel injection or enema composed of glycerine one ounce, epsom salt one ounce, and enough soapsuds to make a pint is often helpful.
Hygienic Measures.—These are of the utmost importance. Diet should be nutritious and easily digested. Milk is the ideal food. If peptonized it is more readily digested. Fermented milk known as koumiss, is excellent. Meat juice is highly nutritious. Meat broths are stimulating but do not contain a large quantity of nutriment. Soups strained and skimmed may be borne. As a patient grows better, he may take soft eggs, custard, junket, rice pudding, milk toast, boiled chops, oysters, and so forth.
|
|
|
|
|
|
|
The Sick Room.—The sick room should be bright and well ventilated. The temperature 68 degrees Fahrenheit. Bed clothing should be clean, the patient should be sponged daily for cleanliness and to keep the skin active. A little alcohol added to the water makes a grateful sponge bath.
Antipyretics.—Antipyretics are agents reducing temperature. If fever is excessive, it is best lowered by cooling drinks and the application of cold to the surface. The latter is most usually accomplished by ice-bags, by cold sponging or cold pack.
Stimulants.—In low, long-continued inflammatory fever, some form of alcohol is most essential. It should, however, be given under the direction of a physician only.
Abscess.—An abscess is a newly formed circumscribed cavity containing pus. This new cavity is formed by the liquefying action of the bacteria upon the tissues.
Forms of Abscesses.—The general classes of abscesses are acute, following an inflammation, and that variously called chronic, cold, strumous or tubercular. The latter form is due to the bacillus of tuberculosis, and does not contain true pus.
Acute Abscess.—As soon as it is determined that an inflammation has gone to suppuration, free opening should be made. After free opening and evacuation, an abscess cavity should usually be irrigated by an antiseptic fluid. If free opening has been made, hydrogen peroxide is excellent for cleansing. This should be followed (unless abscess be of an internal organ) by corrosive sublimate solution (1 to 1,000 or 2,000). Drainage by tube or otherwise should be provided and hot moist antiseptic dressings applied. Rest promotes healing. This is obtained by bandages, splints, slings, and so forth.
Chronic Abscess.—The tubercular cold, scrofulous, or so-called chronic abscess, is a cavity produced by the action of the bacilli of tubercle. No true pus is present unless pus organisms have also gained entrance. A cold abscess lacks inflammatory signs. There may be no constitutional symptom unless true suppuration is added. The general health of the patient is, however, invariably below normal.
|
|
|
|
|
|
|
Treatment of cold abscesses is upon the general principles for the treatment of acute abscess, but should be trusted to none but a surgeon.
Felon or Whitlow.—This is a violent rapidly-spreading inflammation of a finger or toe, usually the former, due to pus germs. The symptoms are throbbing pain, great tenderness, swelling, a dusky redness. In case of a deep felon redness and pain may extend up the arm, and there is usually fever.
Treatment.—Rarely the application of iodine, cold, rest and elevation may afford relief. Generally, however, such treatment is worse than useless. Early free incision is very generally the only effective procedure. Incision, irrigation, antiseptic fomentations, and splinting, with elevation of the extremity, is the outline of treatment.
Boiles or Furuncles.—This is the most common form of superficial abscess. If not surgically treated, a boil will finally rupture, pus will flow out, and a "core" of dead tissue at last be discharged. The treatment consists of early crucial incision, removal of dead tissue, irrigation with peroxide of hydrogen and corrosive sublimate, and the application of hot antiseptic fomentations.
Carbuncle.—This condition is a circumscribed infectious inflammation of the deeper layers of the true skin and subcutaneous tissues. It ends in a slough. A carbuncle has many points of suppuration. It often causes profound constitutional disturbance, and may prove fatal in the aged and enfeebled.
Treatment.—The best treatment is that of cutting out, under general anesthesia, the entire area infected. The large wound produced heals by granulation, or may later be skin-grafted. The wound is treated and dressed antiseptically. Secure rest and sleep with morphine, give nourishing diet and attend to the bowels and kidneys.
Ulcers.—An ulcer is a loss of substance (due to inflammation) of a superficial structure. It is commonly known as a "sore." The causes are various. Blows may knock off the skin. Burns may cause extensive ulceration. General diseases, such as tuberculosis or syphilis, may predispose to ulcers. Bed sores are common. Varicose ulcers of the leg, due to enlarged veins, are frequently met with.
Treatment.—Treatment consists essentially of removing the cause, so far as possible, and in treating the ulcer antiseptically. If a bed sore, remove the pressure; if syphilitic, internal medication is imperative; if a varicose ulcer of the leg, daily antiseptic cleansing should be practiced, and aseptic dressing should be applied. The most important factors, however, in assisting nature to relieve the engorged veins are rest, elevation, and firm, smooth bandage from the toes extending above the diseased area.
|
|
|
|
|
|
|
Gangrene or Mortification.—These denote the death of a part of the living body in mass. Putrefaction of the part occurs while it is attached to the living body. Gangrene results from a cessation of blood supply, or from obstruction of the outflow of blood from a part. Common among the causes producing such interference are a feeble heart and hard diseased blood vessels. Other causes are injuries, such as a crush, heat or cold, constitutional disease, such as diabetes.
The aged and enfeebled with hard vessels, should avoid injuries, even slight ones, of the feet. The mere cutting of a corn too closely may lead to gangrene. Such a person should attend carefully to the general health and should especially keep the feet warm and comfortable. The treatment of gangrene demands all the skill of a competent physician.
Kinds of Fracture.—Fractures are classified as of two kinds, the simple and the compound. A simple fracture is one in which the skin is not injured, so that no matter how much the bone is broken up, there is no communication of the fragments with the external air. A compound fracture is one in which the breaking of the bone is accompanied by a wound, caused either by the same force which produced the break, as, for instance, a bullet, or by the ends of the broken bones protruding through the skin. For example, a man may fall from a tree, breaking the femur or large bone of his thigh, and the broken end of the bone may be driven through the skin and into the ground. Compound fractures are much more dangerous than simple ones, chiefly because whenever the skin is broken there gain entrance to the tissues disease-producing germs, which set up the process of suppuration.
|
|
|
|
|
|
|

Treatment.—Compound fractures are also more likely to be serious because the skin and muscles are much bruised. When, however, the wound which communicates with the fracture and makes it compound is small, an effort should be made to gain the advantages of a simple fracture by covering the opening in the skin with a clean cloth wrung out of corrosive sublimate solution (1 to 2,000) or wet with salt solution (one teaspoonful to the pint) until the surgeon arrives and takes charge of the case. This imperfect effort at antiseptic treatment must often fail, from the impossibility of applying it quickly enough, but it ought always to be tried.
|
|
|
|
|
|
|
Recognizing Fractures.—"We may recognize the fact that a bone is broken by the following indications: first, that the limb is shortened or bent where there is no joint; second, by there being an unnatural degree of movement at the seat of injury; third, by the violent pain which attends a fracture; fourth, by the grating which may be felt, and sometimes even heard, when the limb is moved.
Setting of Broken Bones.—This consists merely in pulling and pressing the fractured extremities of the bone into their proper position. Such an operation, of course, requires a full knowledge of the anatomy of the parts and should, as a rule, be left for a skillful medical attendant, if he can be procured, within twelve hours. In the mean time the wounded part should be placed in the most comfortable, or rather the least painful, posture, wrapped in cloths wet with laudanum, or lead-water and laudanum, and kept cold with ice, in order to prevent swelling and diminish the suffering as far as possible.
Keeping a Broken Bone in Place.—When the physician succeeds in replacing the fragments, his next object is to secure them from being again deranged. This is usually accomplished by the aid of splints of various kinds, such as are shown applied to the arm on the opposite page. These splints may be made of wood, tin, pasteboard, or gutta percha, and are kept in place themselves by bandages or knotted handkerchiefs. In certain cases, material, such as plaster of Paris or starch, which stiffens after it is applied to the limb, upon a bandage, can be employed with great advantage.
Injuries Far from Home.—When a person is injured far from any habitation, and must be moved a considerable distance, if it is found that a bone has been broken, the first thing to do is to apply to the fractured limb a temporary splint. This will prevent the injury from becoming compound, if it is as yet only a simple fracture, and will save the wound from being irritated, if the injury is already a compound one.
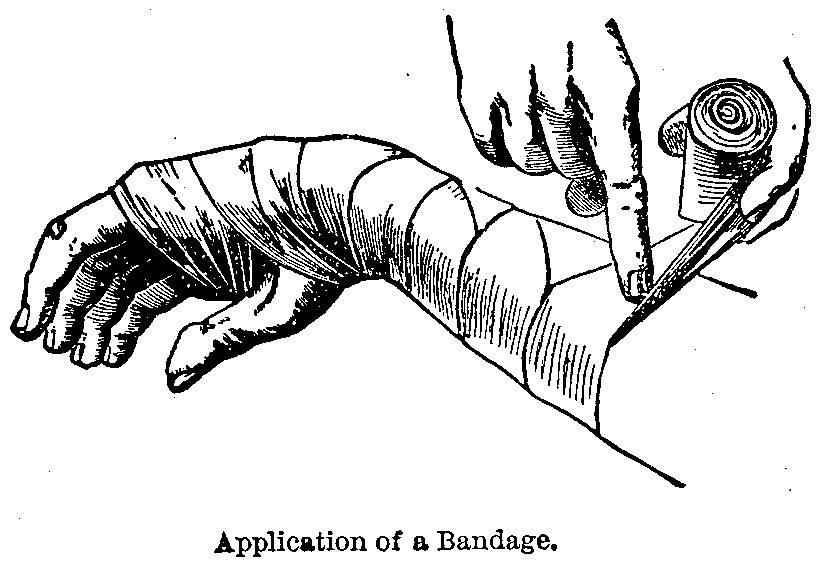
Bandaging.—For the making of bandages and the various kinds see conclusion of this article. The operation of bandaging requires some practical experience before it can be performed neatly. The idea, however, of the method of procedure, winding the cloth smoothly around the arm, for instance in a spiral direction, can be gathered from the illustration. Where the limb is conical, increasing in size from below upward, the only way to cause the bandage to lie evenly and be of much use is to make what are technically called reverses, turning the roll of linen over each time as it comes on top, as is represented in the wood cut. The artist, however, has delineated the surgeon's fingers as being those of a left-handed man, a variety of the human species which, strange to say, is tenfold more numerous in pictures than in real life. The best substitutes for bandages available at a distance from human habitations are often to be found in handkerchiefs.
|
|
|
|
|
|
|
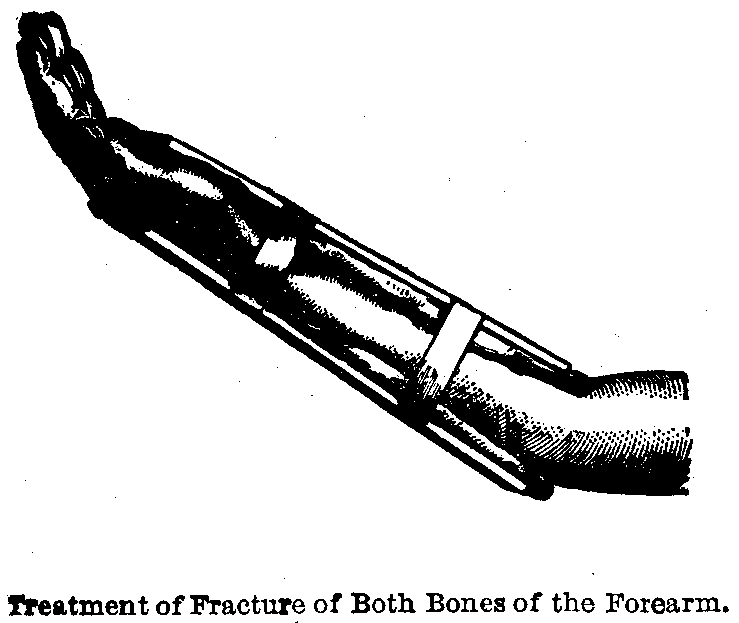
Splints.—To obtain splints for the temporary support of fractures, the most varied articles have been pressed into service. Thin, light boards, like shingles or the sides of a cigar-box, which can be cut into any form desired, are often the best, but any object which may be trimmed or bent to suit the exigencies of the case, and is stiff enough to retain the form given to it, can be utilized. After preparing the splint it should be padded, for which purpose cotton-batting, tow, old rags, dried leaves, or hay may serve, these materials being bandaged fast to it on the side which is to Come in contact with the injured member. The apparatus is then applied to the limb, an arm, for example, as shown in the figure below, and after carefully adjusting the injured member to the least painful position, as well as to that which is nearest its own natural shape, the splint or splints are fastened in place with several turns of the bandage applied as previously suggested. The adjoining woodcut shows the method of applying the splints for a fracture of both bones of the forearm. After arranging the arm and splints as depicted, the whole should be covered in with a bandage, and suspended by a sling from the neck in such a way as to be carried by the patient across his chest.
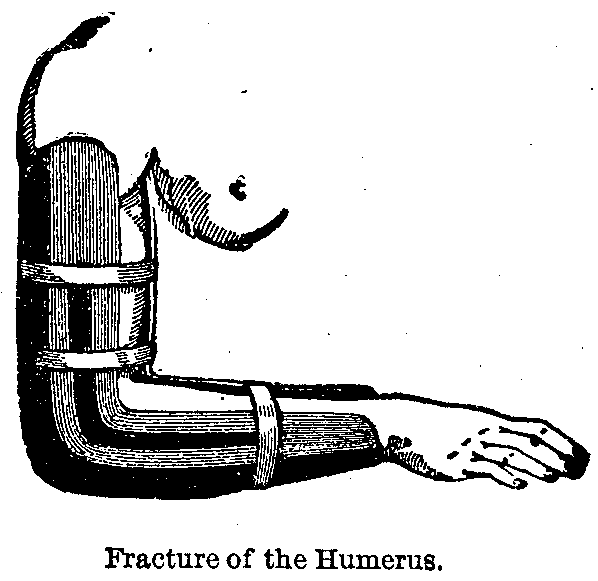
Fracture of Arm.—Fracture of the humerus or arm-bone between the shoulder and elbow should have applied curved splints made of thick pasteboard, wet in boiling water and moulded to the shape, sheet gutta percha similarly softened, or tin, one on the inside and another on the outside, as represented in the figure. The fragments of the bone are to be adjusted in proper position, a bandage applied, and then the splints fitted and firmly yet not too tightly bound on with a bandage running from the tips of the fingers to the shoulder. If the roller is applied above only, the hand and fingers will swell up in consequence of the pressure, interfering very seriously with the circulation of the blood. In fractures of the arm it is always advisable to arrange the elbow bent at a right angle, because should the arm be left stiff, as may happen, perhaps with the best treatment, it is much more useful than when straight.
|
|
|
|
|
|
|

Fracture of Legs.—In fractures of the legs, a contrary rule holds good, and the effort should always be to keep the broken limb as straight as possible.
An excellent temporary dressing for a fracture of the leg below the knee is well indicated in the figure. The injured limb should be drawn out to as nearly its full length as can be borne, measuring it by the sound side to determine this, and then the fragments of the bone pressed, if possible, to their proper places. The pillow which has previously been laid beneath the injured member is then doubled up, as shown in the cut, and fastened with three or four strips of bandage or with handkerchiefs. If the leg is much bruised, or the pain very severe, a soft linen cloth soaked in laudanum, or strong lead-water and laudanum, should be wrapped around it before being bound up in the pillow.
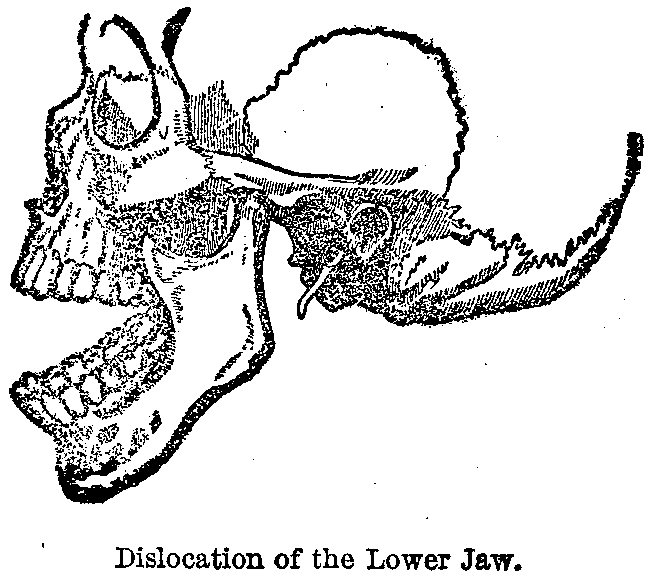
Dislocations.—Continued displacement of the bones comprising a joint, after the ligaments have been more or less torn, constitutes a dislocation, or, as it is popularly described, "out of joint." These injuries are generally the result of external violence, such as falls, blows, twists, and so forth, which have caused the limbs to move in a direction, or to an extent, for which nature had not adapted them. A familiar example of a dislocation is that of the lower jaw, and the position of the bones composing this important articulation in their disturbed or displaced condition is well shown in the marginal illustration.
|
|
|
|
|
|
|
Symptoms of Dislocation.—In a general way, a dislocation is recognized, first, by the altered appearance of the joint, which is usually very apparent when compared with the corresponding joint on the opposite side; second, by the movements of the affected joint being lessened; third, by the fact that efforts to move the joint cause much pain; fourth, dislocation can usually be distinguished from fracture, which, when near a joint, is apt to give rise to all these symptoms, by the absence of crepitus, as the grating noise produced by rubbing together the ends of the fragments is called. This sign, however, would, of course, prove fallacious and misleading if both a fracture and a dislocation existed.
Treatment.—The obvious treatment for a dislocation is reduction, or a replacing of the bones forming the joint again in their proper relations. In reducing a dislocation, not only should the operator have all his anatomy at his fingers' ends, but a vast amount of practical experience is often necessary to decide whether a dislocation is complicated with a fracture, or whether a dislocation or a fracture is the injury to be treated.
So great and so permanent is the injury likely to result from the blunders of attempting to "reduce" a fracture, erroneously supposing it to be a dislocation, or vice versa, that no time should be lost by the sufferer in availing himself of the best medical services procurable.
Sprains.—Sprains are injuries resulting from the twisting or tearing of the ligaments of a joint by the effects of a fall or blow. Sometimes the violence of muscular action, or the sudden weight of the body, brought to bear upon a joint when unexpected by the antagonistic muscles, may be the cause of a sprain. The pain is frequently very sharp and severe, and swelling takes place with great rapidity. The most common sprain is that of the ankle, and its effects are so speedily manifested that in the course of a few minutes the patient becomes unable to walk or even put his foot to the ground without great suffering.
|
|
|
|
|
|
|
Treatment.—Recovery from a sprain takes place slowly, and the serious mistake is often made of considering the injury a trifle. Perfect rest is essential. An affected ankle should be elevated above the hip. For the first few hours ice-water cloths should be held upon the joint by a firm pressure bandage. An ice-bag should be added. After some hours the extremity should be placed upon a splint. Cold applications of water, lead-water and laudanum, or of alcohol and water should be continued. Leeches about the joint do good. Dover's powder for pain may be necessary. Use the constitutional treatment for inflammation. After a day or two hot fomentations with the hot water bag give greater relief. When the pain and other acute symptoms have well subsided, gentle motion and rubbing with liniments help to prevent stiffness. Time is lost by attempting to use the affected limb before it is sufficiently restored.
Foreign Bodies in the Throat.—Foreign bodies in the throat are sometimes substances imprudently swallowed by mistake, such as fish bones, pins, and so forth, or coins, marbles, and other playthings half ignorantly introduced by children. If the breathing is not seriously interfered with, medical assistance, sent for at once, should be awaited, as peculiar forceps and other instruments will probably be necessary to extract the intruders. If choking to death seems imminent from pressure on the windpipe, thumping on the back, holding the patient up by the heels, and striving to hook out or push the foreign body, if it is not intrinsically dangerous, down into the stomach, may all be tried. At the last gasp the operation of tracheotomy, or opening the windpipe, should be performed by any one who has the knowledge and the courage to attempt it.
Foreign Bodies in the Nose.—Foreign bodies in the nose are generally beads, buttons, beans, and so forth, pushed up by children with the usual desire to see what they will do. They may sometimes be driven out by violent sneezing excited by snuff, or by tickling the inside of the nostril with a feather. If such treatment is not effective, the case should be referred to a physician, who can as a rule readily remove such objects with suitable instruments.
Foreign Bodies in the Eye.—Should a particle in the eye lie beneath the lower lid, it can generally be extracted by pulling down the eyelid, searching out the object by the aid of a bright light and a magnifying glass, and wiping it off with the corner of a fine handkerchief, or with a little brush made by gently twisting a bit of absorbent cotton on the end of a wooden toothpick. Objects beneath the upper lid are more difficult to manage. If the popular mode of wiping the inside of the upper lid with edge of the lower one over which it is drawn down, fails to give relief, the lid should be at once turned inside out. This little operation is performed by taking hold of the eye-lashes, pulling out the lid from the eye, and having the patient look down at his feet just as you press the back part of the lid down with a bodkin or small lead-pencil laid across it above the eye. The particle will generally be found adhering to the under surface of the lid, and, when detected, should be removed as before advised.
|
|
|
|
|
|
|
Foreign Bodies in the Ear.—Foreign bodies in the ear, including insects, may generally be removed by syringing with plain boiled tepid water. This is far safer than to attempt to remove objects with instruments. Should an insect gain entrance to the ear and no syringe be at hand, let the patient lie down upon the opposite side and fill the auditory canal with warm water. This will kill the insect and may float it out of the canal.
Burns and Scalds.—Even when small and slight, the suffering produced by burns is severe; when extensive, they are dangerous, and if the whole body is involved certain death is the result. Burns are caused by fire, or by chemical agents applied directly to the surface, destroying the skin, and, to a greater or less extent, the tissues underneath. Scalds are produced by the contact of boiling liquids or steam. The three degrees of a burn are, first, mere painful redness, caused by superficial inflammation of the cutaneous surface; second, the formation of blisters; third, charring of the skin, and, perhaps, of the deeper structures. Probably the most frequent cases of fatal burning are from the clothes taking fire.
When the Clothing Takes Fire, the person, if alone, should throw himself flat upon the floor, and strive to smother the flame by wrapping around him a rug, shawl, coat, or any woolen article within reach. If any other person is present, he should instantly trip or knock down the sufferer, and use his coat or the first woolen article which comes to hand to smother out the fire; then procure water as quickly as possible, and drench the patient with it. In the terrible cases which occur where the entire body is one vast blister, the best way is to give a large hypodermic injection of morphia, or a full dose of laudanum, and roll the patient in a sheet after covering the body with sweet oil and dusting it with flour.
Treatment.—For the local treatment of slight burns, including sunburns, nothing gives more relief than that of wrapping the part in cloths kept wet with a strong solution of baking soda or dilute phenol-sodique (one to eight parts of water). Carron oil (a mixture of lime-water and linseed oil), or an application of white-lead paint, relieve pain, but are apt to be followed by much suppuration.
|
|
|
|
|
|
|
Severe Burns.—In severe burns an effort should be made to dress antiseptically. Cleansing should be done by sponging with hydrogen peroxide, following with boric acid solution, or a solution of common salt, one teaspoonful to the pint of water. Blisters should be pricked with an aseptic needle. One of the most grateful dressings is that of soft cloths kept wet with the salt solution. Or, after cleansing as suggested, the wound may be dried and dressed, boric acid powder and plentiful dry aseptic absorbent cotton being applied. Carbolized sweet oil may be used. Burns from falling into a lime-kiln or a kettle of soap-lye should be treated with plenty of cool water, and then washed with diluted vinegar, except where the skin is broken, to neutralize the alkali; afterwards, the burns which remain are to be dressed as directed for those which have been produced by fire. Burns from acids, such as nitric acid or oil of vitriol, should, on the contrary, be treated by profuse washing with lime-water, a solution of baking soda, or any other alkali which can be procured.
Extensive burns are very dangerous and require the attention of a physician to direct constitutional as well as local treatment.
Frost Bite.—A sufferer from frost bite should not be suddenly brought into a warm room. A frost bite should be gently rubbed with snow or ice-water cloths, thus reëstablishing the circulation gradually. The part should later be wrapped in cotton wool and should be put at rest in an elevated position.
Injuries by Electricity.—Whether electrical shock be by lightning-stroke or by artificial current the treatment is similar. Make traction upon the tongue and artificial respiration as directed under the subject of Anesthesia. Do not give alcoholic stimulants. Apply cold to the head, apply a mustard plaster to the back of the neck and another over the heart. Wrap the patient in warm blankets and give rectal injection of hot salt solution. If a person is in contact with a live wire, first, if possible, shut off the current. If this cannot be done catch a portion of the clothing of the victim and pull him away from the wire; or handle him with rubber gloves or by wrapping the hands in dry cloths.
Rupture or Hernia.—By the above is commonly meant the protrusion of some organ of the abdomen through the walls of the latter. The most common contents of hernia are bowel or omentum. The commonest sites are at the navel and the groin.
|
|
|
|
|
|
|
The fact that persons so affected are often induced to entrust themselves to the treatment of quacks or charlatans is deplorable. Serious results often occur. There are only two forms of proper treatment, namely, either the wearing of a truss fitted and adjusted by a skilled person or submission to surgical treatment at the hands of a reputable surgeon for the radical cure of the condition.
|
|
|
|
|
|
|
Apparent Death from Vapors.—When a person is overcome by illuminating gas or other noxious vapor he should be quickly removed from its presence into fresh air. The clothing should be loosened, the tongue drawn out and rhythmical traction be made upon it. The mouth and throat should be wiped free from mucus. Artificial respiration should be practiced. Meanwhile external heat should be applied and active stimulation given hypodermically or by the bowel. If respiration begins to be restored oxygen should be given by inhalation.
Apparent Death from Hanging.—After cutting the patient down the principles of treatment are similar to those applied in the case of asphyxiation from vapors.
Ivy Poisoning.—This is a condition caused commonly by the poison-oak or poison-ivy. It is characterized by redness, burning, itching and generally by swelling with a vesicular eruption.
Valuable applications are those of cloths wet with lead-water and laudanum, black wash or phenol-sodique one part, water eight parts. Mild ointments give relief, especially oxide of zinc ointment containing ten grains of carbolic acid to the ounce.

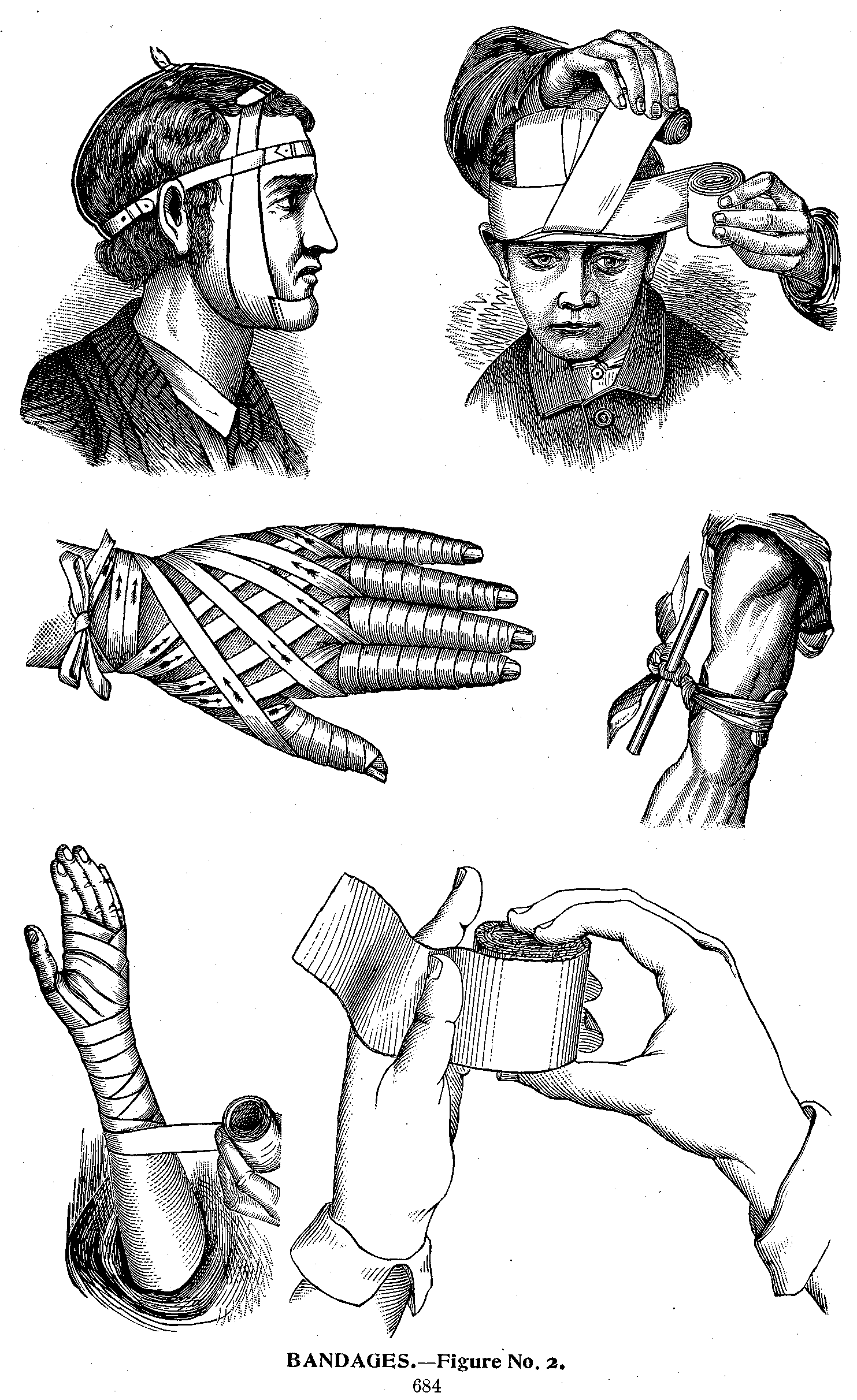
Bandages may be made of gauze, cotton, flannel, rubber, muslin, etc. They are used to hold splints or other dressings in place, to give support, to make compressions, and to correct deformity. When desirable to -have a part absolutely rigid starch, silicate of sodium, plaster-of-paris or like material may be incorporated in the bandage.
Bandages are named from their shape, use, mode of application, from a fancied resemblance to something, or from the name of their inventors.

The Roller Bandage (Fig. 2) is usually made of unbleached muslin which has been washed in soda solution to remove the sizing and then torn into strips varying from one to five inches in width and from three to ten yards long, according to the part to be bandaged.
|
|
|
|
|
|
|


The cut (Fig. 1) represents the simplest and best variety of machine for rolling bandages. It consists of a framework, through the upper part of which passes a square bar (rounded where it corresponds to the uprights) with a handle attached. The strip of muslin being spread out, one end is passed beneath the lower bar seen in the cut, and then over the upper one, which being turned by the other hand, soon rolls the whole bandage. After it has been rolled up, it should be seized with the left hand and held firmly while the crank is turned in the same direction, so as to still more tighten up the bandage. Then reverse the crank which will allow the spindle to be withdrawn.
The bandages may also be rolled by hand. The edges should be kept true, the loose threads picked off, and the end of the bandage secured with a pin.
The T Bandage (Fig. 3) is made by sewing one piece of bandage at right angles to another, is used to retain dressings between the thighs. One part of the bandage is tied around the waist, the stem of the T passing between the legs, then being brought up and tied to the first part.
The Many-tailed Bandage (Fig. 4) is used principally after abdominal operations. On applying it the central portion is placed over the spine and beginning at the top, the first tail on one side, then the first tail on the opposite side is brought across the abdomen, so alternating and overlapping until all the tails are used.
|
|
|
|
|
|
|
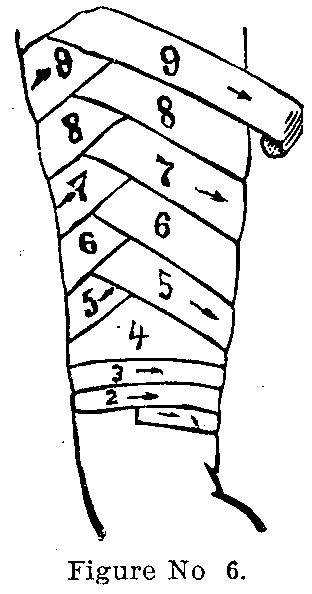
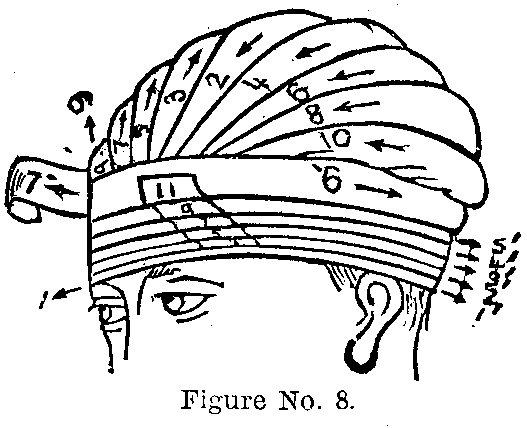
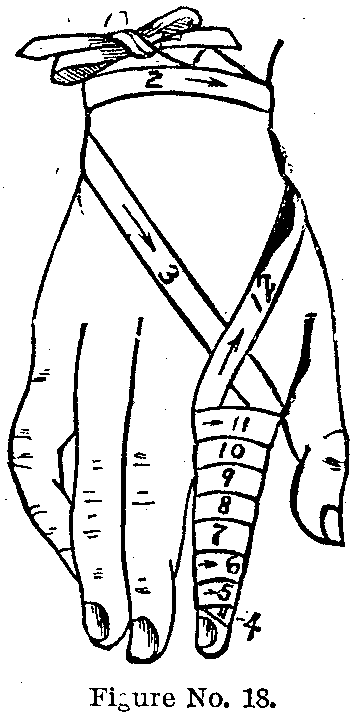
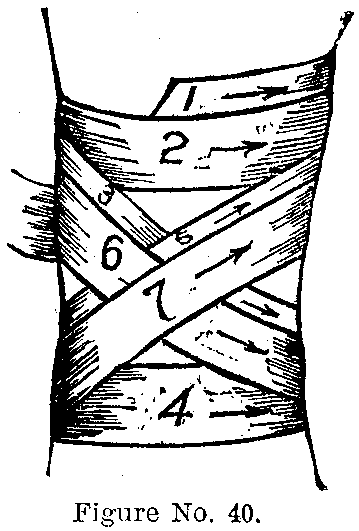
The Maltese Cross is used to retain dressing on stumps after amputation of a limb, the ends folding smoothly over the operative field.
The Circular Bandage consists of several circular turns around a part and is used to stop hemorrhage, make veins prominent before blood-letting, and to retain dressings when limited to small area.
The Recurrent Bandage is applied to various parts. To adjust it to the head make several turns around the head (Fig. 8), then pass the bandage backward and forward over the scalp until the parts are covered. Secure the turns with pins or strips of adhesive plaster.
The Oblique Bandage is begun by several circular turns and is then carried up the limb like the red band on a barber pole. It is rarely used.
The Spiral Bandage (Fig. 18) is applied to parts which do not vary in circumference. It is applied like the oblique except that the turns overlap each other. Figure 33 illustrates the spiral bandage applied to the chest. Figure 24 demonstrates the application of the spiral bandage to the hand and wrist.
|
|
|
|
|
|
|
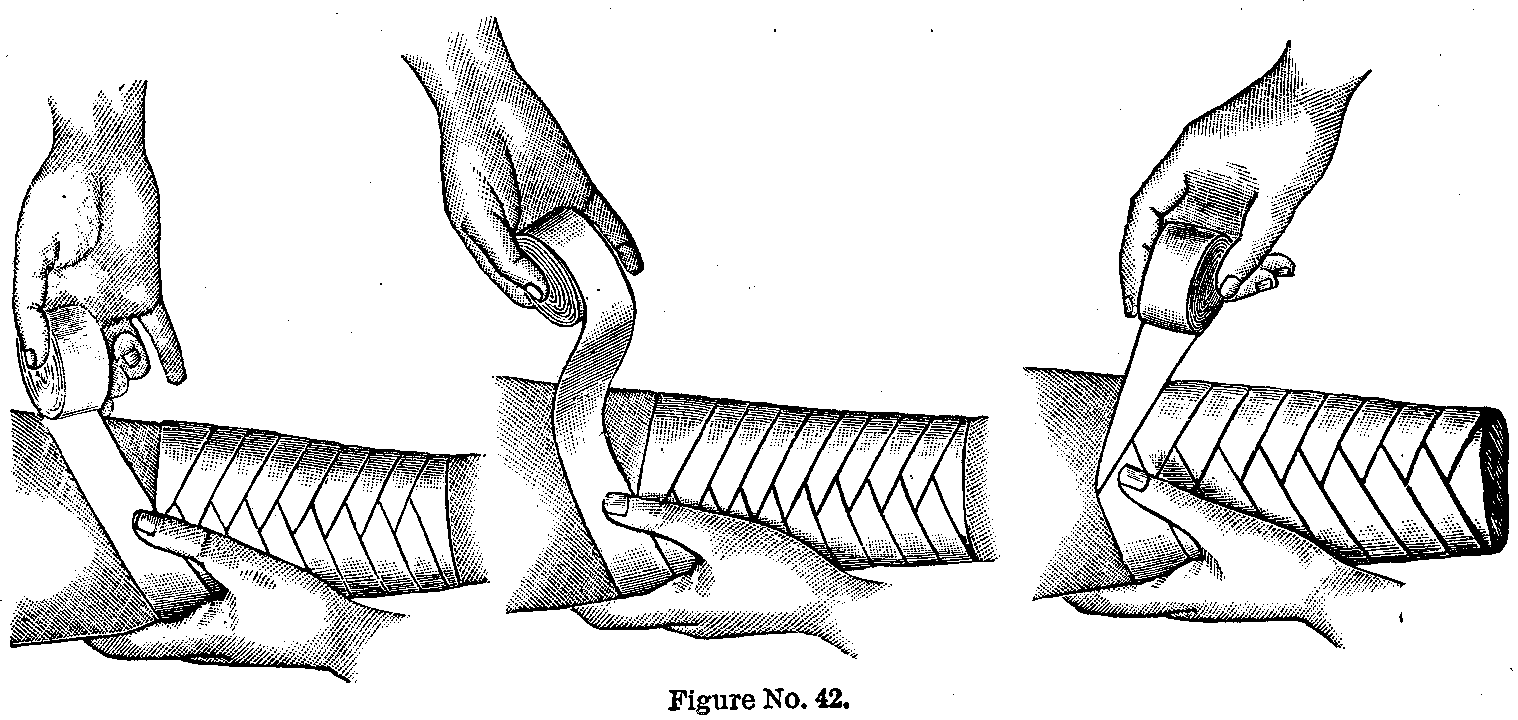
The Spiral Reversed Bandage (Fig. 42) is applied to parts which are conical. It is begun like the spiral, but as the leg begins to thicken it will be found that the lower edge of the bandage does not lie snugly against the limb. In order to obviate this reverse each turn of the bandage, i. e., the upper edge of the bandage becomes the lower edge. Overlap each preceding turn of the bandage at least one-half.
To confine the bandage the end should be folded on itself, the corners again folded under and a pin should be passed in the direction from which the end of the bandage has come.
The Figure of Eight Bandage is applied to the knee, elbow, chest, axilla and occiput. Make several circular turns around the limb to fasten, pass obliquely downward over the flexor side of the joint to the opposite side, make a circular turn below the joint, and pass obliquely up again. The figure of eight is repeated, overlapping the turns until the part is covered.
Figures 12 and 13 show the method of applying the figure of eight to the eyes to retain dressing, exclude light, and so forth.
Figure 20 shows an excellent method of binding up the hand and wrist by means of a folded handkerchief in times of emergency. Care should be taken not to allow any tight constriction around the wrist for a prolonged period, as death of the fingers may result.
|
|
|
|
|
|
|
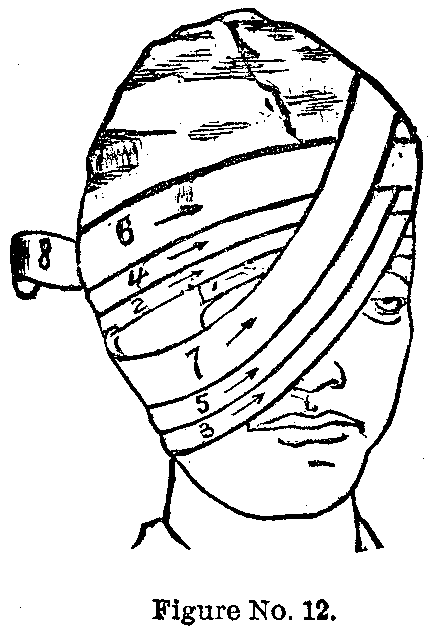
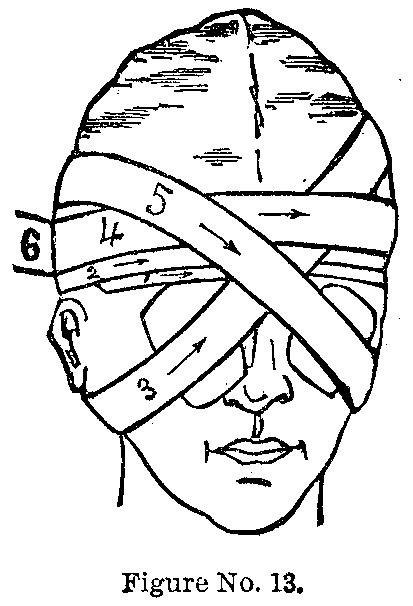
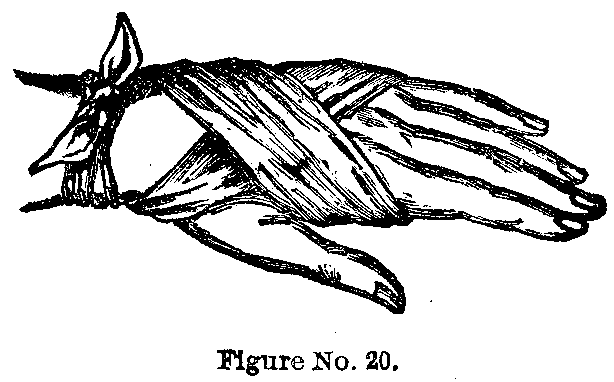
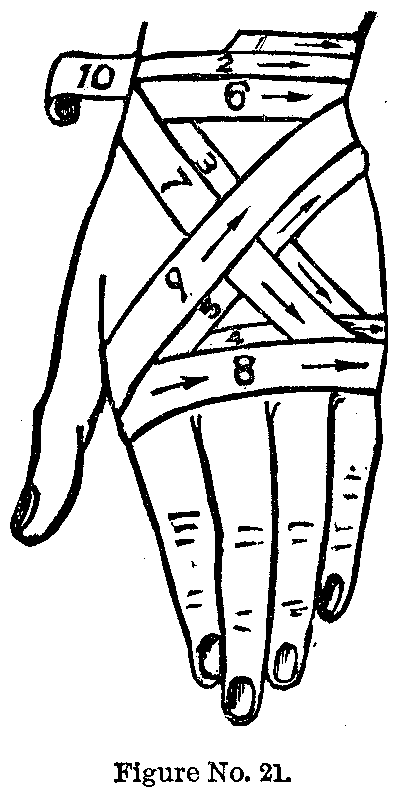
In Figure 21 the same principle, the figure of eight, is utilized to cover the back of the hand and wrist.
In Figure 37 the figure of eight is employed to cover the instep.
The bandage is fastened by circular turns above the ankle, and is then applied as above described.
The Spica Bandage is a figure of eight bandage, each turn overlapping the previous one so as to resembled[sic] a spike of barley. When the turns overlap each other from below upward the bandage is called an ascending spica; when from above downward, a descending spica. When the turns cross in front it is termed an anterior spica; in back, a posterior spica; and on the side, a lateral spica; when two corresponding parts like the groins are covered, the bandage is known as a double spica.
|
|
|
|
|
|
|

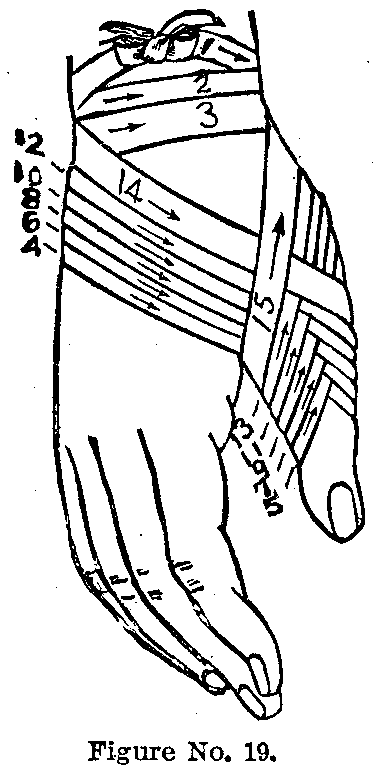


The Four-tailed Bandage is made by taking a square or oblong piece of flannel or muslin, and tearing toward the centre from opposite sides, so as to make four tails. The size depends on the size of the part to be covered.
Figure 9 illustrates the four-tailed bandage adjusted to the head.
For the instep make the bandage about twenty inches long and about five inches wide. Double it and tear down the centre, leaving a square portion untorn. Apply it by placing the central square portion across the instep; bring the two upper ends up around the leg and tie them; the lower ends are to be brought about the lower part of the foot and tied in a similar manner. This bandage is very effective in confining dressings to the instep and lower part of the leg. It may also be applied to the heel.
|
|
|
|
|
|
|
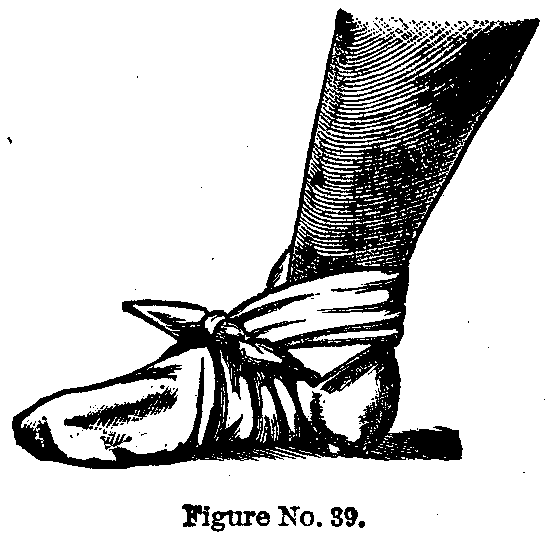

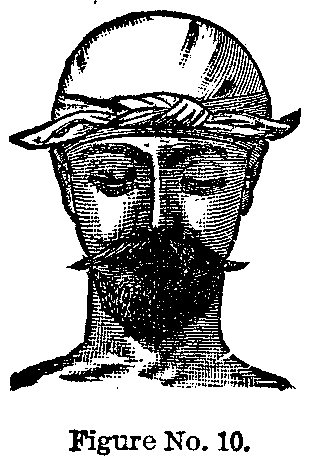

For the knee take a strip of muslin eight inches -wide and about thirty inches long; tear each end down the middle to within six inches of the centre. Apply the central portion over the patella, bring the upper ends of the bandage around behind the knee, passing obliquely downward, and tie on the front of the leg below the knee pan; the lower ends should be crossed behind in a similar manner, and tied on the front of the thigh above the knee pan.
|
|
|
|
|
|
|
Figure 15 shows the four-tailed bandage applied to the chin.
The Triangular Bandage by skillful manipulation has been made to perform many and varied offices.
Figure 10 shows the ordinary triangular bandage applied to the scalp in a manner somewhat like that adopted by women to protect the hair from dust when sweeping.
In Figure 26 the methods of binding the shoulder, elbow and hand are shown, as well as the use of the triangular bandage for a sling.
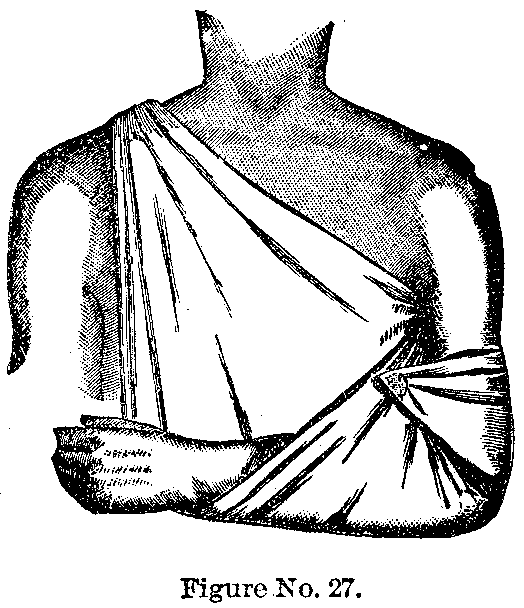
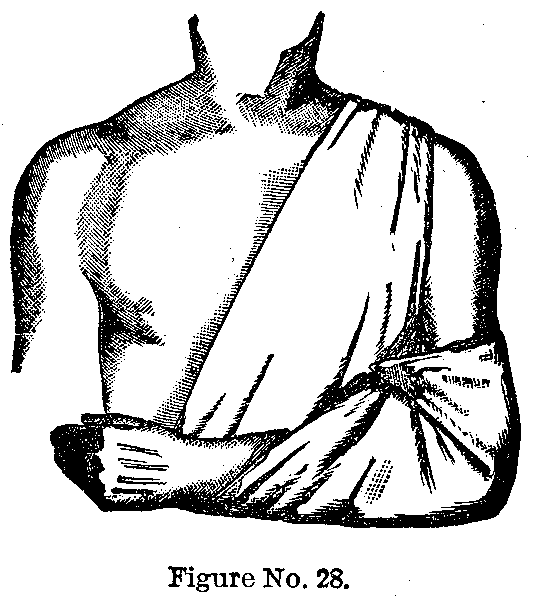

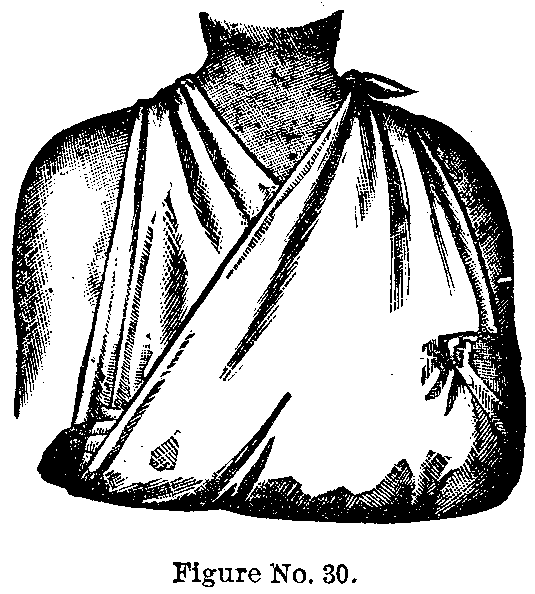
|
|
|
|
|
|
|
In Figure 27 the triangular sling is so adjusted as to support the arm and elbow, the weight resting on the right shoulder only.
In Figure 28 the same bandage is depicted, except that the weight of the forearm falls on the left shoulder.
In Figure 29 the bandage is so applied that it cannot be removed by a child or restless patient.
Figure 30 shows the triangular sling applied in the usual way, the weight being supported by both shoulders.
Figure 31 shows the triangular bandage applied to the chest, shoulder, head and elbow.



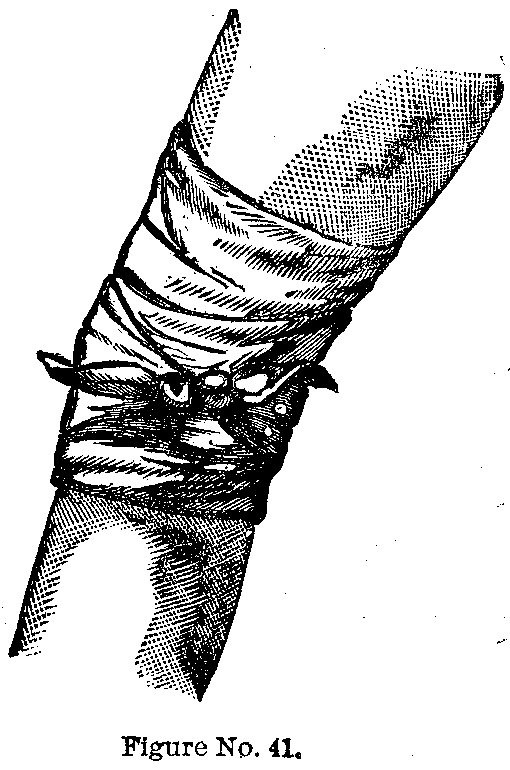
|
|
|
|
|
|
|
In applying the triangular bandage to the knee take a triangle of muslin, the base being about two feet long and the apex about ten inches from the base. Place the centre of the base across the front of the knee just above the knee pan; bring the ends around as many times as possible and tie them. Dressings are easily held on by this method, and much support is given in cases of fracture of the knee pan.

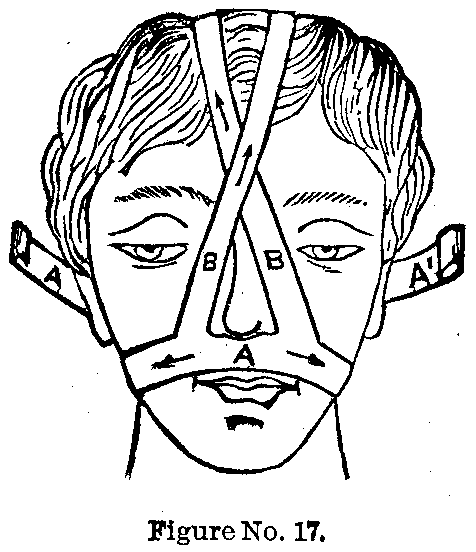
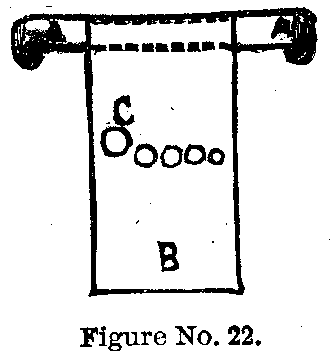
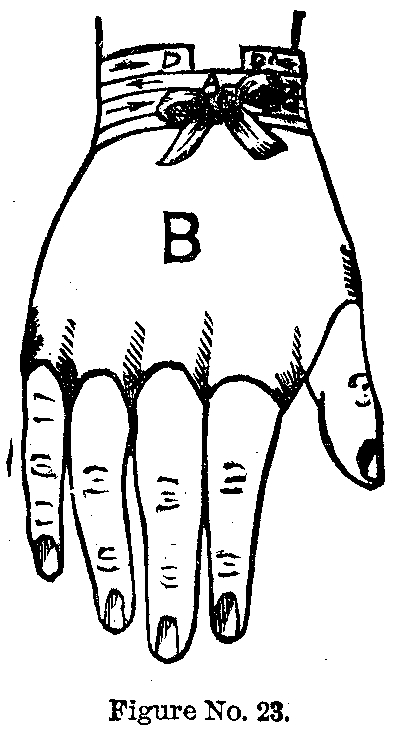
The Fillet or Head Band.—Take a piece of flannel twenty-five to thirty inches long and about ten inches wide. At the centre of the bandage, one-half inch from the lower edge, cut a triangular hole large enough for the nose. Stand behind the patient and place the bandage over the face, the nose projecting through the hole, the remainder of the upper part of the face being covered. The ends are brought together behind and pinned. This is an admirable dressing for retaining dressings on the face and eyes, especially in burns of the face.
|
|
|
|
|
|
|
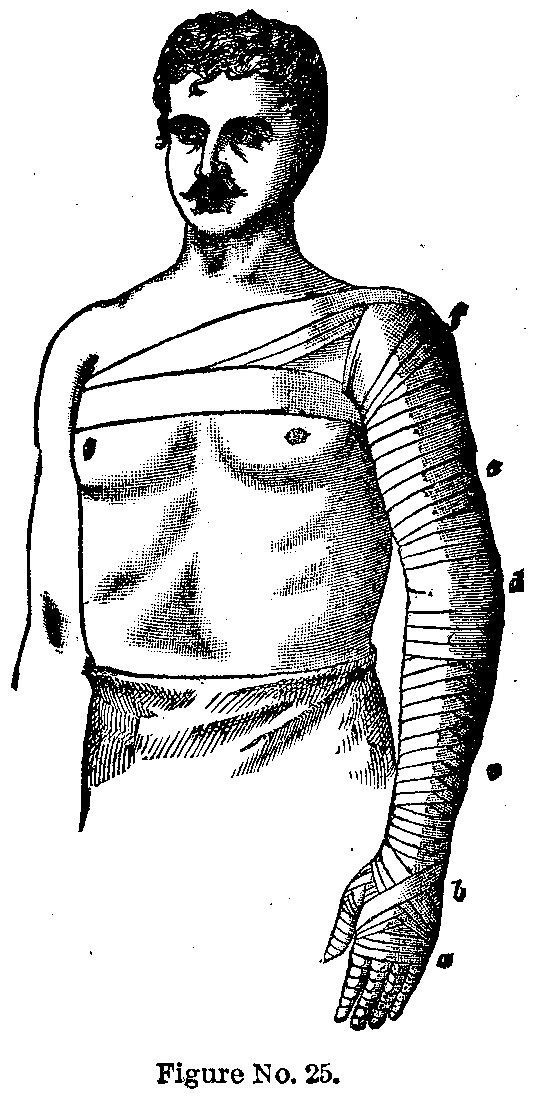
Bandage for the Chin.—This bandage should be one and a half inches wide and about nine yards long. Standing at the back of the patient, the end of the bandage is placed just over the left eyebrow, and fastened by one horizontal turn around the head, then passing around to and below the right ear, underneath the chin, and upward over the left side of the face, Just covering the left ear. Two more turns are to be made over the top of the head and underneath the chin, each turn including a little more of the anterior part of the chin. The bandage is now to be continued around behind the neck, and, in a slanting direction, over the head and around the forehead, as before, and then again below the right ear and across the front of the chin and around the neck, drawing this part quite snug, and repeating; then passing under the chin and up on the left side of the face, bring the bandage to the top of the head and confine by several turns.
|
|
|
|
|
|
|



It is used for fracture of the lower jaw, and for holding poultices to the side of the face, and so forth. If any turns be made about the neck, care should be taken that they are not drawn tight enough to interfere with the circulation.
T-Bandage for the Temple.—Take two pieces of muslin, one two to four inches wide and three feet long; ten to twelve inches from one end, at right angles to it, another bandage should be fastened, two inches wide and seven to eight feet long, one end only extending fifteen to eighteen inches beyond the point of junction.
|
|
|
|
|
|
|
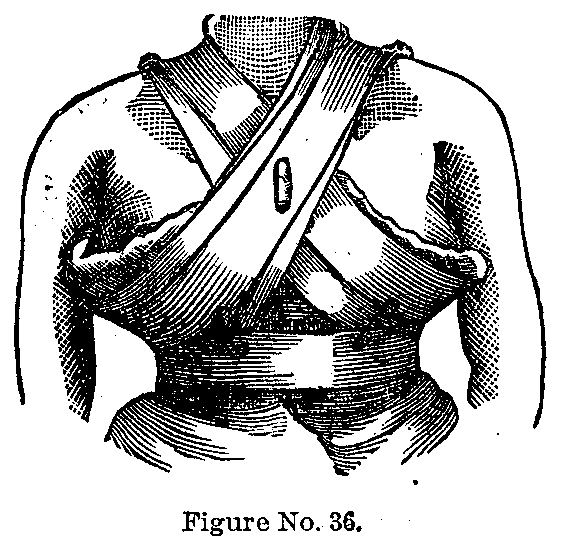
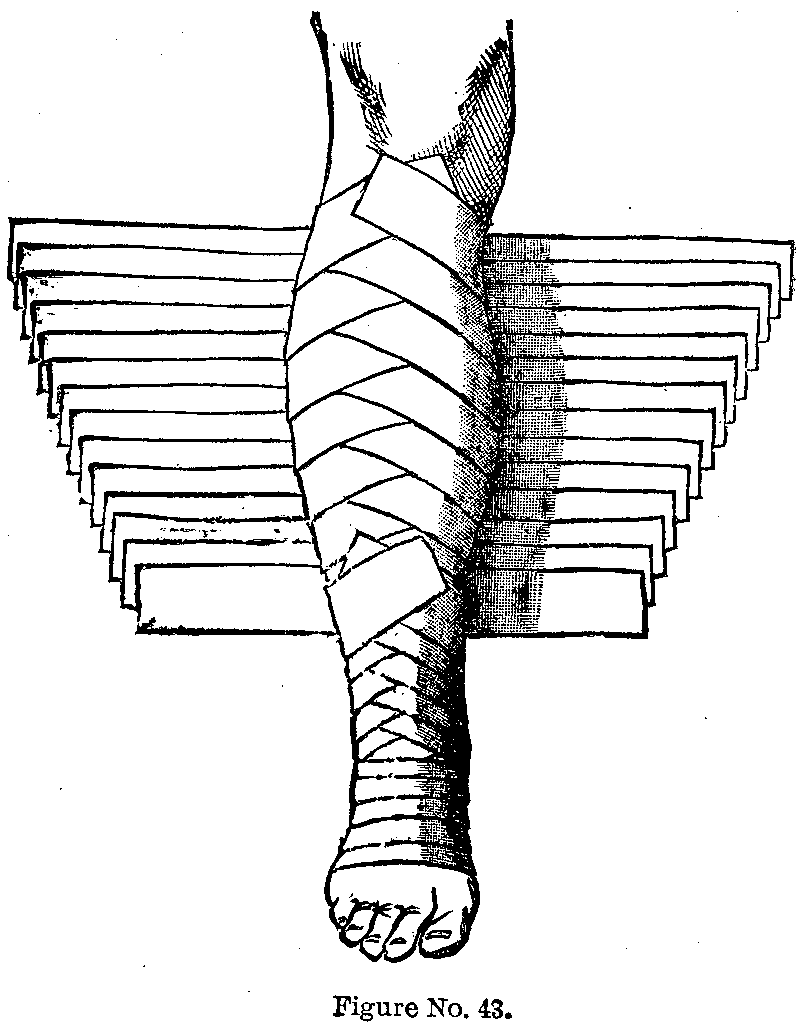
Place the point of junction of the bandage over the injured temple in such a manner that the wide part of the bandage is perpendicular as regards the head; the short end is to be brought to the top of the head and the long end around under the chin and fastened to the opposite end. The narrow part of the bandage is now carried around the head horizontally, the short end being confined by the horizontal turns.
Double T-Bandage for the Nose.—Take a muslin bandage seven to eight feet long and one inch wide. At the centre of this, about one inch from each other, and at right angles to the first, stitch two other strips each two and one-half feet long by three-quarters of an inch wide.
Place the centre of the main bandage beneath the nose (the two shorter pieces passing up on each side, crossing at its base and resting on the top of the head), carry the ends around to the back of the head where they cross and are again brought around to the forehead, where they may be confined after taking several circular turns about the head. The ends passing over the top of the head may pass down behind and be pinned to the main bandage. This bandage is of use in keeping dressings about the nose in position.
|
|
|
|
|
|
|
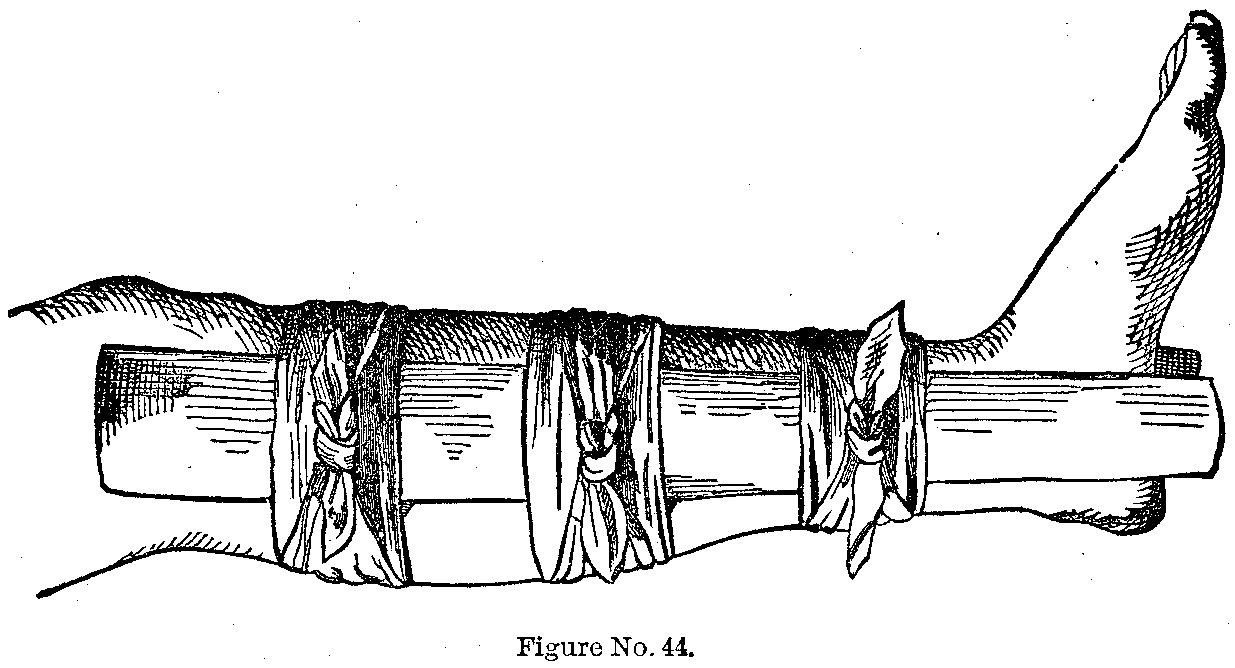
Perforated Bandage for the Hand.—Take a roller bandage eighteen inches long and one inch wide, and to the centre of this stitch a piece of linen one foot long and four inches wide, with five perforations, as in Figure 22.
Pass the thumb and finger through the holes, double the ends over the wrist and secure with the roller bandage.
Figure 25 shows how the whole upper extremity may be covered by bandaging. Each division of the arm may be taken separately to show the method of applying a bandage to any part of the arm.
Figure 32 shows a very useful apparatus for applying continuous cold. to an inflamed member; it may be just as easily applied to the head or lower extremity. It consists essentially of a vessel with ice water, a rubber tube and a support for the arm.
Bandages for the Breast.—We will assume the left breast is to be supported.. It is first covered with a layer of cotton; then applying the end of the bandage about the centre of the back, holding it in place with one hand and with the other bringing the roller under the arm and breast, then across the chest and over the right shoulder, then under the arm and breast again until it is covered; the bandage should now pass across the chest at the level of the lower end of the breast-bone, below the opposite breast, and around behind, where it may be confined.
When both breasts are to be supported the bandage should pass across the left shoulder also and below the right breast in the same manner.
Figure 43 shows the manner of covering the leg with adhesive plaster cut in strips, each strip being longer than the preceding and overlapping it. Pieces of bandage may be used in making a many-tailed bandage.
|
|
|
|
|
|
|
Figure 44 shows how a fractured limb may be put up temporarily by using two straight pieces of wood and several handkerchiefs. The limb should be covered with cotton or some other soft substance.
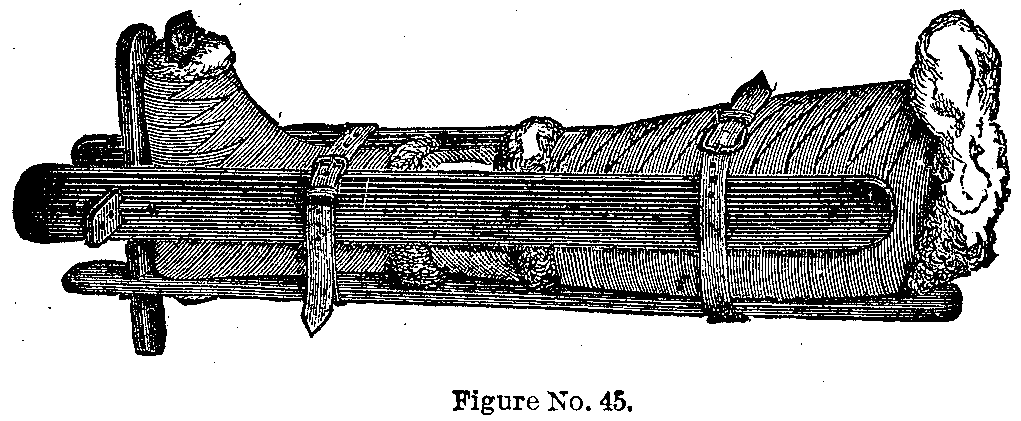
Figure 45 shows the construction and use of a very efficient apparatus for the leg, especially when the fracture is of the compound variety.
This page is maintained by
Charles Keith.
Contact:
Send me a message
Last Modified: Monday, 13-May-2013 15:31:47 EDT